Study design
This study is a randomized, double-blind, placebo-controlled multicenter III study. The study followed the Declaration of Helsinki and Good Clinical Practice guidelines. Written informed consent was provided by all patients, and the protocol and amendments were approved by all sites’ institutional review board and independent ethics committee.
Patients
Key eligibility criteria wereage ≥18 years;histologically confirmed SCLC not previously systemic therapy for ES-SCLC that classified by the American Veterans Association for Lung Cancer; Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1; estimated survival time >8 weeks; at least one measurable lesion according to Response Evaluation Criteria in Solid Tumours version 1.1 (RECIST v1.1); adequate organ and bone marrow functional reserves; provision of tumor samples for biomarker PD-L1 assessment.
The main exclusion criteria include: history of autoimmune diseases; Received CTLA-4 inhibitors, PD-1 inhibitors, PD-L1/2 inhibitors, or other drugs targeting T cells; Brain metastases that require treatment; Use corticosteroids or other immunosuppressants within 14 days prior to randomization; clinical symptoms or diseases of the heart that cannot be well controlled; uncontrolled active infections; other malignant tumors occurred less than 5 years before randomization.
Randomization and blinding
Eligible patients were randomly assigned to two groups in a 1:1 ratio. The general information of eligible patients were input into the Randomization and Trial Supply Management provided by an independent third party for randomization. Stratified block randomization (block size: 4) was adopted in this study. Random assignment was stratified by gender (male or female), ECOG PS (0 or 1) and brain metastasis (yes or no). Socazolimab and placebo were consistent in appearance and shape. The patients, investigators, and sponsors or their designated personnel were not aware of the grouping.
Procedure
Socazolimab (5 mg/kg) or the corresponding placebo were treated intravenously every 21 days until disease progression, intolerable toxicity or death, or up to 2 years. In the chemotherapy regimen, carboplatin was given once within the area under the serum drug concentration time curve of 5 mg/mL/min (AUC 5) on the first day of each 21 days cycle, and etoposide was given continuously with 100 mg/m2 on the 1st, 2nd, and 3rd day of each 21 days cycle. The treatment of EC regimen was used until the completion of 4 cycles, with disease progression, intolerable toxicity, or death. During the treatment, the dose of reduction or suspension of EC was allowed, but socazolimab or placebo was only allowed for dose suspension up to 12 weeks. All dose modifications methods were shown in protocol. The main reason for choosing placebo combined with EC as the control group is that EC remains the recommended first-line treatment for ES-SCLC in China during the study design.15
During the research process, radiological examinations were conducted every 6 weeks or as deemed necessary by the central investigator,, and radiological evaluation was performed by the investigators and Independent Radiology Committee (IRC) respectively, but it was only up to the investigators to decide whether to continue treatment according to the evaluation results of the investigator.
Outcomes
The primary end point of this study was OS, defined as the time from randomization to death. Key secondary outcomes included PFS (progression-free survival, defined as the time from random assignment to disease progression or death from any cause), ORR (objective response rate, defined as the proportion of patients with a complete response or partial response to treatment) and DoR(duration of response, defined as the time from onset of response to progression or death due to any reason, whichever occurs earlier) assessed by investigators or IRC based on RECIST v1.1, and OS rates at 1 and 2 years, adverse events, the association between PD-L1 expression levels in tumor tissues and efficacy, and other secondary outcomes including immunogenicity and quality of life that were not reported here.
Adverse events were recorded up to 90 days after the last dose of the entire study treatment and scored using the National Cancer Institute’s Common Terminology for Adverse Events (version 5.0). Treatment-related adverse events (TRAE) were defined as adverse events associated with either carboplatin, etoposide, socazolimab or placebo. Adverse events related to the use of ICI therapy are defined as immune-related adverse events (irAE).
Expression of PD-L1 was assessed by immunohistochemical method in formalin-fixed, paraffin-embedded tumor samples. The analyst stained PD-L1 positive paraffin tissue with PD-L1 antibody (Anti-PD-1 28-8) and used its isotype control antibody (Recombinant Rabbit IgG) as a control to confirm the specificity of the antibody and determine non-specific staining and/or background staining in the tissue.The definition of PD-L1 positivity is that tumor cells with partial or complete membrane staining account for at least 1% of the total live tumor cells.
Statistical analysis
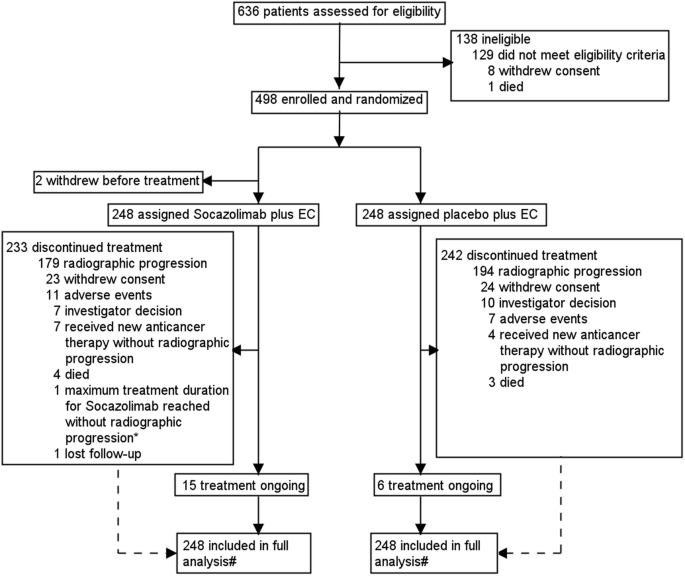
The calculation of sample size for clinical trials is based on the primary endpoint of OS. An estimated 5% patient dropout rate per year is planned to include 498 eligible patients. Assuming a median OS of 10.5 months for the placebo plus EC group and a required number of deaths of 369 to provide 85% of the detection power, the HR for death between the socazolimabplus EC group and the control group is set at 0.73 (based on CASPIAN study result.7)
An interim analysis was planned when ~222 (60% of the 369) expected deaths had occurred, a α-spending function of O’Brien-Fleming type is used to control the overall type I error rate. The final analysis would initiated when the cumulative number of deaths reaches 369. At the actual interim analysis cutoff date (March 20, 2023), As of the actual mid-term analysis deadline (March 20, 2023), there were 225 deaths (61.0%) (significant level, one sided p = 0.0041). In the interim analysis, compared with the placebo plus EC group, the HR of death in the socazolimab plus EC group was 0.73 (95%CI 0.56–0.96; one sided p = 0.0109), and did not reach the predetermined superiority boundary. Based on these results, the Independent Data Monitoring Committee recommended that the trial be continued according to the original design. As of October 13, 2023, there were 382 deaths and a final analysis of the OS was carried out, with the one-sided alpha value for hypothesis testing is 0.0236. The final statistical analysis results are presented here.
The full analysis set was used for efficacy evaluation, including all randomized patients who have received ≥1 study drug treatment. Among the patients included in the full analysis set, those with safety assessment data were all included in the safety analysis set.
The Kaplan-Meier method was used to estimate the efficacy endpoints, including OS, PFS, and DOR, and the 95% CIwas calculated using the Brookmeyer Crowley method. The survival data between the two groups was calculated using a stratified log rank test. Estimation of heart rate and 95% confidence interval using a stratified Cox proportional hazards model (gender, ECOG PS, and brain metastasis as stratification variables, treatment group as a covariate). Based on age, gender, ECOG status, brain metastasis, liver metastasis, disease stage, and PD-L1 expression, a stratified Cox proportional hazards model was used to conduct pre planned subgroup analysis of survival benefit indicators, including OS rate and PFS rate. The number and proportion of patients who achieved objective response in each group were calculated, and 95% CI of response rate was calculated based on Clopper Pearson method. Cochran-Mantel-Haenszel (CMH) chi-square test (gender, ECOG PS, and brain metastasis as stratification variables) was used to compare the objective response rate between two groups.



留言 (0)