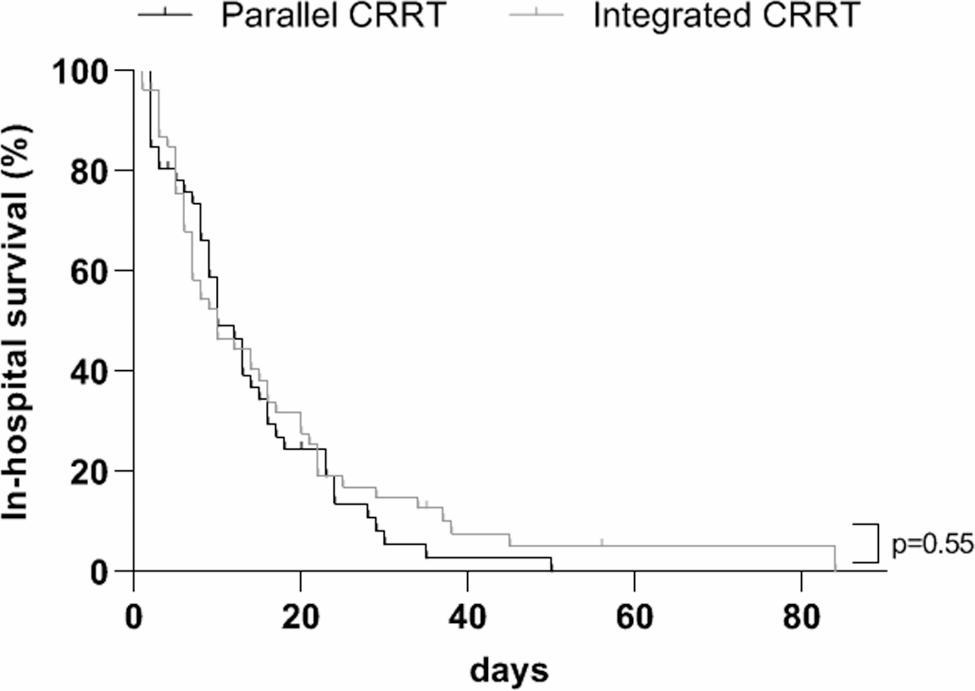
Our retrospective study demonstrated that integrating CRRT into the ECMO circuit in 57 patients had a safety and efficacy profile comparable to that of the independent parallel CRRT and ECMO configuration in 48 patients. There were no significant differences in in-hospital mortality between the two modes of CRRT and ECMO connection, nor did they significantly impact on the length of stay in the intensive care unit. The integrated delivery approach was not associated with a significant increase of complications (e.g., haemolysis, CRRT or ECMO machine failure, CRRT or ECMO tubing leaks, pressure alarms in either extracorporeal system), filter clotting, or the need for CRRT circuit changes. Both approaches showed no differences in the course of the patients’ laboratory values, and CRRT settings remained stable during therapy using the two different connection modes.
To date, there are no definitive guidelines recommending which combination technique should be used in ECMO patients with AKI requiring concomitant CRRT [3]. Any integration of the CRRT circuit directly to the ECMO circuit is not officially approved by the Food and Drug Administration nor by the manufacturers, and clinical practice is primarily based on expert opinion and local experience [3, 6, 15]. Two recent multicenter international surveys reported that up to 60% of centres used an integrated in-series approach, while only 40% of units used the parallel connection technique (16–17). Currently, there have been few comparative studies with small sample sizes on this issue [6, 15].
Independent central venous vascular access is required for the parallel conduction of CRRT and ECMO (2–3, 6, 15). Given the systemic heparinisation and prolonged coagulation time in ECMO patients, it has been suggested that this approach is associated with an increased risk of bleeding, particularly with invasive central venous catheter placement (2–3, 6, 11, 15). However, our analysis did not show a significantly increased incidence of bleeding in the PAG. In fact, there was a slight trend towards a higher frequency of bleeding events in the IAG. In general, catheter site bleeding was rare. The majority of bleeding events were non-serious and occurred in the otorhinolaryngological area. However, all of the few cases of pulmonary bleeding were documented in the IAG. Both groups had comparable platelet counts and coagulation values at baseline, and initial anticoagulation strategies were similar for both approaches. The increase in aPTT and INR during support was observed at similar levels in both groups. However, the IAG experienced a greater decrease in platelet count at the end of therapy than the PAG, which may have predisposed them to observed higher rate of pulmonary bleeding. At the same time, four cases of systemic thromboembolism in our study were also reported only in the IAG, which contrasts with previously reported higher rates of systemic thromboembolism in the parallel use of CRRT and ECMO (2–3, 6, 15, 18). In general, ECMO population is prone to thromboembolism because of the overexpression of cytokines related to the ECMO support, which induces activation of the coagulation cascade [19,20,21]. In addition, ARDS due to COVID-19 pneumonia is often associated with thromboembolic events driven by thromboinflammation [22]. Endothelial dysfunction, dysregulation of the innate and adaptive immune systems leading to overwhelming production of proinflammatory cytokines, and platelet hyperactivation leading to release of large amounts of chemokines and subsequent activation of the complement system and the coagulation cascade are key pathological responses of thromboinflammatory processes that contribute to thrombus formation during SARS-CoV-2 virus infection [22].
Contrary to the assumption of an increased risk of infections with parallel CRRT connection using an additional central venous catheter, we did not observe any differences in central venous catheter-associated infections or bacteraemia in our study cohort (2–3, 6, 15). Regarding other potential complications of the parallel approach requiring additional vascular access, we observed a pneumothorax in only one patient in the PAG after central venous dialysis catheter insertion, and no vascular injury. The creation of a central venous access is a challenging and potentially limited procedure when two vascular access sites are concurrently utilised by ECMO [3]. In certain cases, the introduction of a third vascular access may be necessary to achieve the required blood supply for the ECMO support [3]. Additionally, a number of anatomical or pathological scenarios (e.g. vascular anomalies, thromboses, skin infections in the vascular access area) can limit the installation of a venous access for an independently running CRRT. In such clinical scenarios, a combination of both extracorporeal procedures will inevitably need to be considered, weighing the risks and benefits. Running the CRRT and ECMO systems independently from one another may also require deeper sedation and patient restraint to reduce CRRT alarms, which may contribute to additional complications and exacerbate patient discomfort [3].
Haemolysis due to shear stress and wall impact forces is frequently observed in ECMO patients [23]. The research group of Chen et al. proposed a higher incidence of haemolysis when using ECMO as a direct venous access for CRRT due to the higher pressure in the CRRT circuit in this setting [24]. In the case of two separate circuits for CRRT and ECMO, there is no interference of ECMO haemodynamics with the CRRT machine, theoretically placing the patients at lower risk of haemolysis (2–3, 6, 15). In our study, suggestive haemolysis parameters such as bilirubin and LDH significantly increased, and platelet counts significantly decreased towards the end of supportive treatment; however, there were no relevant differences between the two groups. Haemoglobin levels did not change during support with either CRRT configuration. Therefore, our results did not confirm the previously reported increase in haemolysis in patients with an integrated CRRT connection.
The studies by de Tymowski et al., Crosswell et al., Raja et al. and Wu et al. described significantly higher filter lifespans in their integrated ECMO and CRRT configuration than in their parallel configuration (11–12, 25–26). The findings of our study indicate no statistically significant differences in filter lifetime between the two groups, regardless of the CRRT connection mode. Following the initiation of CRRT, 40% of patients required a system change before the routine 72-hour change. Filter clots were identified as the reason in 30% of cases across both groups. We speculate that the combination of systemic heparin anticoagulation and local citrate anticoagulation, used in more than 90% of patients in both modes, may have prevented early filter clotting in both groups. Giani et al. described that the combination of unfractionated heparin and citrate led to significantly fewer filter changes than the use of unfractionated heparin alone [27]. Otherwise, both CRRT connection techniques have practical drawbacks that could potentially provoke clotting and shorten the lifespan of dialysis filters. On the one hand, problems with central venous dialysis catheters, including catheter strain due to repositioning or other catheter manipulations, as well as disconnection due to transfer to operating theatres or computerised tomography scans, are common reasons for alarms and iterative stops, which interfere with maintaining stable CRRT blood flows and achieving high ultrafiltration fractions, leading to premature filter clotting (2–3, 6, 15). On the other hand, potential exposure of CRRT access and return lines to inappropriately high pressures that are incompatible with CRRT pressure thresholds in ECMO-integrated CRRT is associated with technical problems and CRRT machine pressure alarms, which additionally result in repeated interruptions of CRRT sessions with subsequent reduction in filter lifespan and dialysis efficacy (2–3, 6, 15).
Post-pump settings were utilised at our centre, with the understanding that recirculation in the dialysis circuit is negligible. In our integrated approach group (IAG), the drainage pressure corresponding to the outflow pressure of the ECMO pre-oxygenator segment did not exceed the maximum range of the venous pressure alarm of 300 mmHg over the 7-day follow-up, contributing to an acceptable frequency of clotting and unplanned CRRT system changes. Transmembrane pressure (TMP) was also maintained within an acceptable range of 20–40 mmHg. The ECMO blood flow in our integrated CRRT connection group was moderate between 4 and 5 L/min, which may have also protected against the development of higher outlet pressures in CRRT lines above the safety threshold of 300 mmHg. The pre-oxygenator pressure range increases with higher ECMO blood flows (maximum ECMO flow is 6 L/min) [13]. The oxygenator traps air bubbles and clots, which is a major advantage of this integrated CRRT configuration chosen in our centre [3, 9]. Accordingly, no cases of air or blood leakage were observed in the IAG of our study. Based on our data and in agreement with previously published work, we think that connecting the CRRT inflow line to the return ECMO line after the oxygenator and the CRRT outflow line to the drainage ECMO line just before the oxygenator is an optimal solution for running CRRT on ECMO. This allows for a well-tolerated venous outlet pressure within the safety range of a maximum of 300 mmHg, thereby not affecting blood flow in the CRRT circuit, and provides an efficient dialysis dose without downtime [3, 11,12,13]. In general, ECMO blood flow rates are lower in veno-arterial ECMO than in veno-venous ECMO [6]. Therefore, we assume that the aforementioned integrated CRRT connection method to the oxygenator should be particularly recommended for CRRT integration into veno-venous ECMO.
We recognise several limitations of our study, such as its retrospective design, which is prone to selection and information bias. Selection bias may be introduced by the non-randomised choice of the CRRT configuration by the ICU and nephrology teams. For example, it is conceivable that patients at high risk of bleeding or with limited vascular access options were predominantly allocated to the IAG, whereas patients who were intolerant of anticoagulation or prone to thromboembolic events were predominantly allocated to the PAG. Some important laboratory values for the assessment of haemolysis, such as haptoglobin, were either unavailable or lacking in the majority of ECMO patients. In addition, the high mortality rate of 89% in both groups may have introduced a mortality time bias. In other words, the effects of different dialysis configurations are overshadowed by the severity of the disease and its high mortality. The small number of survivors insufficient to detect medium to long-term CRRT configuration-specific effects, as the patients will have died of the disease before. Therefore, a larger number of patients who could be successfully weaned from ECMO would be needed in a future study to provide more robust statistical confirmation of our reported equivalent complication rates between the two dialysis configurations. However, the strengths of our study include the relatively large number of subjects in both CRRT connection groups, recruited over a short period without changes in ECMO and CRRT integration practices, and the high homogeneity of the study population, all of whom were suffering from acute respiratory distress syndrome induced by COVID-19 pneumonia.



留言 (0)