Participants
This study was designed as a prospective, randomized, double-blind, single-center controlled clinical trial. It received approval from the Medical Ethics Committee of the Affiliated Hospital of Xuzhou Medical University and was registered in the Chinese Clinical Trial Registry(ChiCTR2400087240). Written informed consent was obtained from all participants prior to enrollment. The study has been reported in compliance with the Consolidated Standards of Reporting Trials (CONSORT) Guidelines, while the protocols were carried out adhering to the principles outlined in the Declaration of Helsinki.
The trial was conducted from July 2024 through September 2024. Inclusion criteria: (1) patients undergoing elective gynecological surgery; (2) American Society of Anaesthesiologists (ASA) grades I-II; (3) aged 18–64 years; (4) BMI of 18–30 kg/m². Exclusion criteria: (1) presence of preoperative oral ulcer, sore throat, throat mucosal injury, or pharyngitis; (2) occurrence of preoperative nausea and vomiting, cough, or dysphagia; (3) history of previous throat surgery; (4) Mallampati grade > 2; (5) patients with hypermagnesemia or hypersensitivity to magnesium prior to surgery; (6) recent respiratory infection before surgery; (7) hypoalbuminemia before surgery; (8) current smoking; (9) placement of a preoperative nasogastric tube; (10) severe cardiovascular, respiratory, liver, and kidney disfunction; (11) treatment with chronic use of calcium channel blockers or magnesium; (12) magnesium sulfate contraindications including acute intestinal bleeding, acute abdomen conditions, pregnancy, and lactation; (13) postoperative intubation was performed again; (14) multiple intubations performed twice or more times during the procedure; (15) durations less than 1 h or greater than 5 h for endotracheal tube placement were excluded from analysis; (16) patients requiring admission to the intensive care unit after surgery.
Randomization and masking
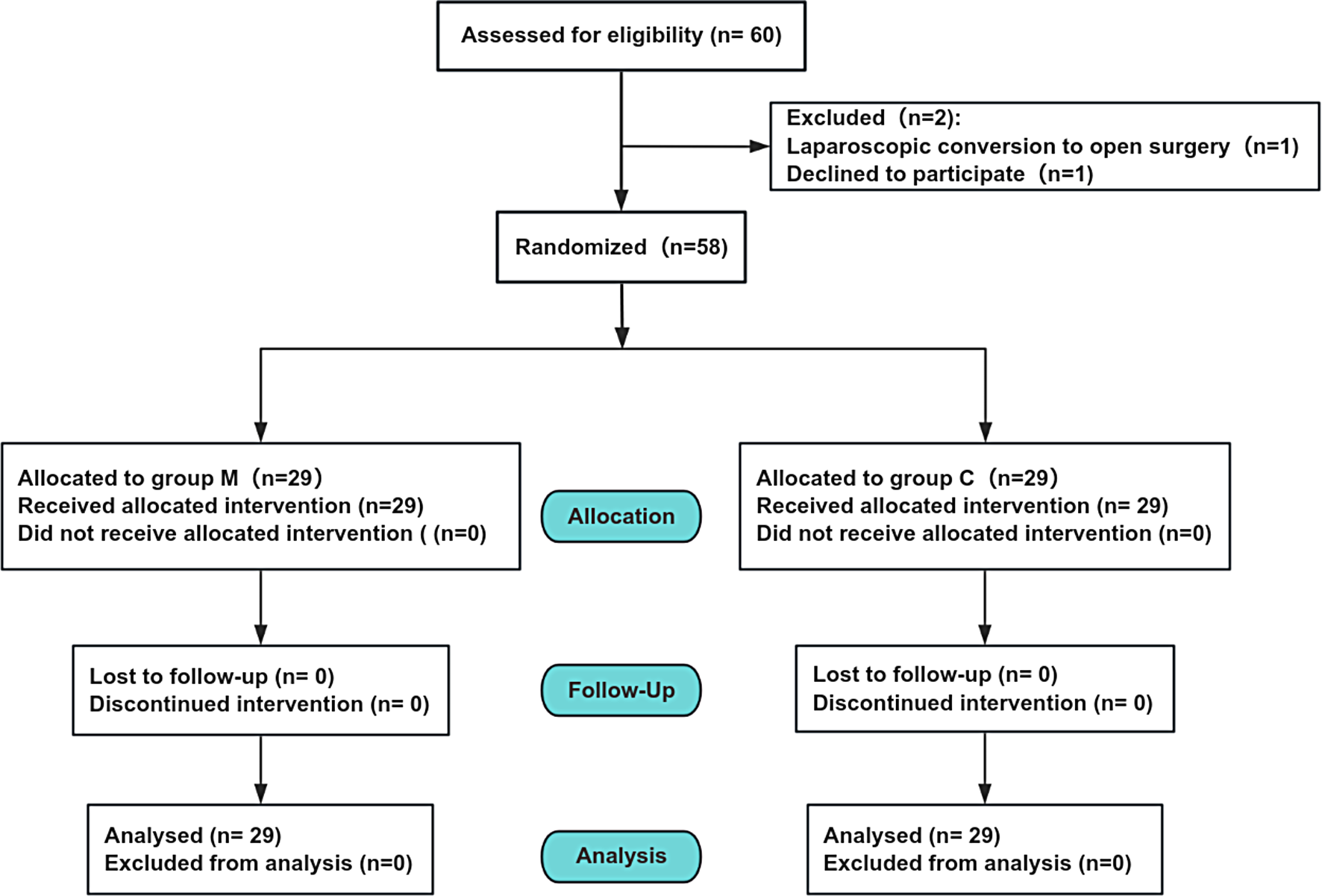
The patients were randomly allocated into two groups: the control group (group C) and the magnesium group (group M) with an allocation ratio of 1:1 according to a computer-generated random number table. A nurse who was unaware of the trial details sealed the group assignments in sequentially numbered opaque envelopes, and the anesthesia nurse opened the envelopes and prepared the trial medications in syringes according to group assignment, with no differences in the appearance of the syringes or medications. Both magnesium sulfate spraying and normal saline spraying, as well as tracheal intubation, were performed by the same experienced senior anesthesiologist. Intraoperative indicators were recorded, followed by postoperative follow-up conducted by another blinded anesthesiologist with respect to grouping assignment, while patients remained unaware of their respective groups. Data analysis of trial results was performed by a statistician who remained unaware of group assignments until completion.
Intervention
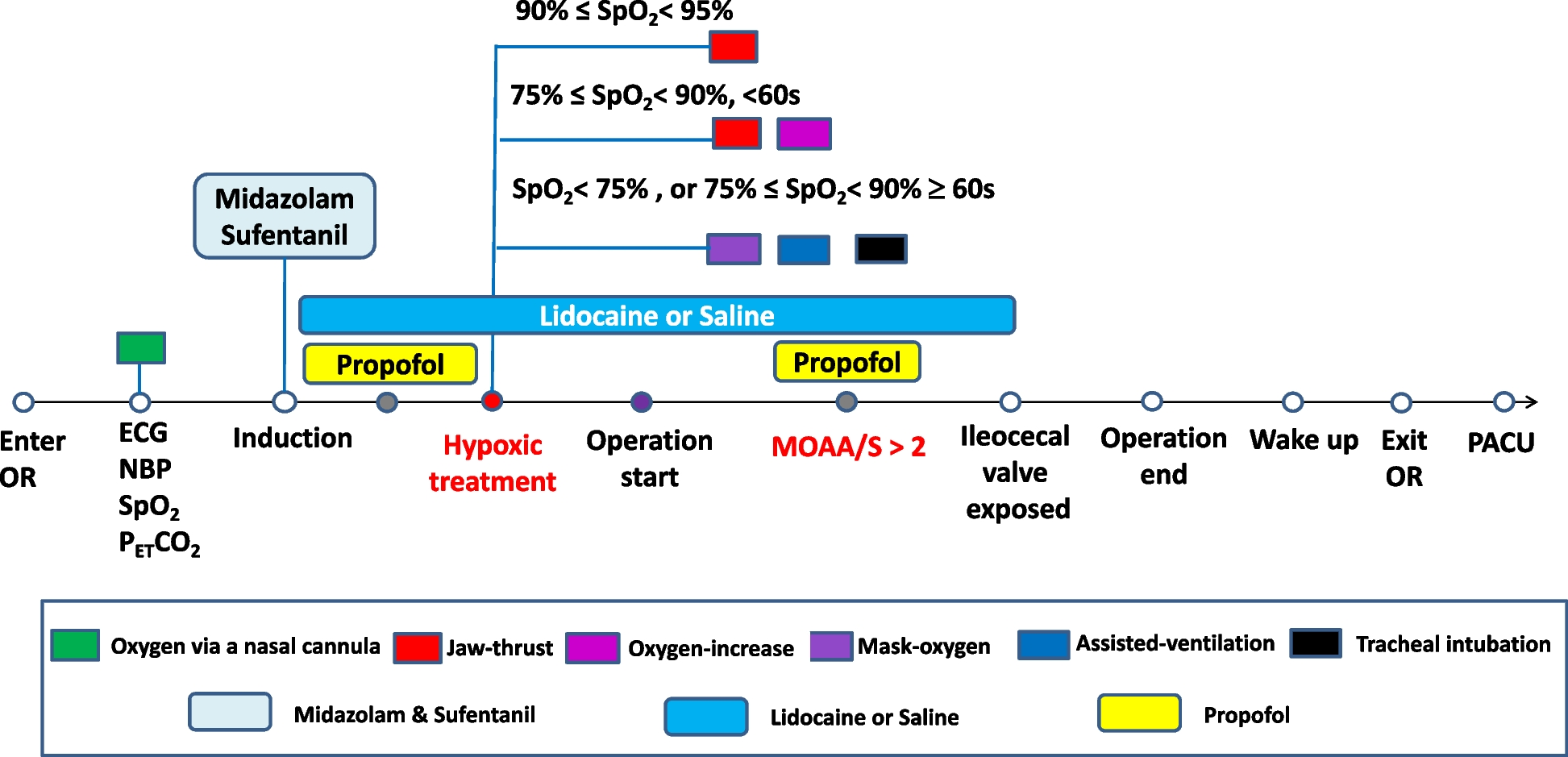
Upon entering the room, routine monitoring was conducted for ECG, BP, SpO2, and PETCO2. Venous access to the upper limbs was established. The Ai anesthesia depth monitor was utilized to monitor anesthesia depth, while the TOF muscle relaxation monitor was used to assess muscle relaxation levels. Anesthesia induction involved a 5-minute preoxygenation period followed by administration of midazolam (0.05 mg/kg), etomidate (0.3 mg/kg), sufentanil (0.5 µg/kg), rocuronium (0.6 mg/kg), and subsequent tracheal intubation.
In the group M, 25% magnesium sulfate at a dose of 15 mg/kg was sprayed onto the mucosa of the pharyngeal region near the vocal cords and the posterior pharyngeal wall using a single-use ear, nose, and throat anesthesia spray device (hereafter referred to as the throat spray) (TUORen Medical Equipment Co., Henan, China) under visualization with a video laryngoscope (administration should be completed within 10 s before intubation). In the group C, an equal volume of normal saline was sprayed onto the same area under the same conditions using the the throat spray. The detailed procedures for drug administration are as follows: The laryngeal anesthesia tube was bent into a shape roughly similar to that of the tracheal tube before insertion, and the epiglottis was not provoked during spraying; epiglottis and the tongue root spray: 1/3, both sides of aryepiglottic fold spray: 1/3, the posterior pharyngeal wall spray: 1/3. The cuff pressure in endotracheal tube maintenance ranged from 22 to 26 cm H2O. Anesthesia maintenance included propofol infusion ranging from 4 to 12 mg/kg/h, remifentanil infusion ranging from 0.2 to 0.3 µg/kg/min, and sevoflurane inhalation maintaining MAC level at approximately 1.3. Throughout the procedure, depth of anesthesia index (AI index) values were maintained between 40 and 60 while blood pressure and heart rate were kept within ± 20% range compared to baseline values. Additional doses of rocuronium were administered based on results obtained from muscle relaxation monitoring to maintain TOF ratio at or above 0. Mechanical ventilation was conducted with a tidal volume of 6-8 ml/kg, an inspiratory/expiratory ratio of 1:1.5, a fraction of inspired oxygen (FiO2) of 60%, an oxygen flow rate of 2 L/min, and the respiratory rate was adjusted to maintain end-tidal carbon dioxide (PETCO2) levels between 35 and 45 mmHg. Administration of propofol and remifentanil ceased at the conclusion of the procedure. Extubation occurred once extubation criteria were met. Upon admission to the Post-Anesthesia Care Unit (PACU), patients were transferred back to their ward upon discharge from PACU.
Outcomes
The primary outcome measure was the overall incidence of POST 48 h after surgery. The secondary outcome included the incidence of sore throat immediately after extubation (T1), at 2 h (T2), 6 h (T3), 12 h (T4), 24 h (T5), and 48 h (T6) after the operation. Sore throat pain scores were assessed immediately after extubation (T1), at 2 h (T2), 6 h (T3), 12 h (T4), 24 h(T5) and 48 h(T6) post-operation using a Numeric Rating Scale [NRS] [13] ranging from scale0(no pain) to scale10(worst pain). The occurrence rate of coughing during extubation. The incidence of nausea and vomiting within 48 h after surgery and the incidence of postoperative dysphagia were recorded. The study also evaluated the incidence of postoperative hoarseness immediately after extubation(T1), at T2(2 h post-op.), T3(6 h post-op.), T4(12 h post-op.), T5(24 h post-op.) and T6(48 h post-op.). Furthermore, the peak airway pressure was evaluated at 5 min, 30 min, 1 h, and 90 min following intubation. Additionally, The Quality of Recovery Scale-15 (QoR-15), was employed to assess the postoperative recovery quality at the 48-hour mark.
Statistical analysis
The sample size was determined using PASS version 15.0, which was based on clinical practice observations and relevant literature research findings. In a previous study, the incidence of sore throat after gynecologic laparoscopy was 69% [14]. In addition, we performed a pilot experiment and showed a 60% reduction in the incidence of postoperative sore throat after magnesium sulfate spraying. Assuming an α level of 0.05, a power (1-β) of 90%, and accounting for a potential dropout rate of 10%, the calculated sample size was 29 per group, resulting in a total sample size of 58 participants.
Data analysis was performed using SPSS software version 26.0. The normality of data distribution was assessed using the Shapiro-Wilk test, while homogeneity of variance was examined using the Levene method. Normally distributed measurement data were presented as mean ± standard deviation, whereas non-normally distributed measurement data were expressed as median (M) and interquartile range (IQR), with comparisons conducted through the Mann-Whitney U test. Generalized estimating equation (GEE) analysis was employed to analyze repeated measurements at each time point within groups. Count data rates (%) were evaluated using either the chi-square test or Fisher’s exact test.



留言 (0)