
記住我


It is a prospective cohort study conducted from June 1, 2019, to July 01, 2021. The study setting was Bahir Dar, in northwestern Ethiopia, 580 km from Addis Ababa, Ethiopia’s capital city. Tibebe Ghion Specialized Hospital (TGSH) was established in December 2018 and offers clinical and academic services through Bahir Dar University. TGSH is a tertiary care hospital that provides medical and surgical services to more than 5 million patients. The hospital currently has over 500 beds and 14 major operating rooms for emergency and elective procedures. Surgical services include general surgery, gastrointestinal and hepatobiliary surgery, urology surgery, neurosurgery, pediatric surgery, head and neck surgery, thoracic surgery, orthopedic surgery, maxillo-facial surgery, ear, nose, and throat (ENT) surgery, obstetrics, and gynecologic surgery. Perioperative surgical services are provided by general surgeons and sub-specialty surgeons in the various units, while master anaesthetists and anesthesiologists offer perioperative anesthesia services. In general, about 1000 health professionals work across the hospital’s many service units.
This study was conducted in line with The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement [17] (See Additional file 1).
Ethical considerationThe Institutional Review Board of Bahir Dar University, College of Medicine and Health Sciences, granted ethical approval to conduct this study (reference number CMHS /IRB 0163/2018). A waiver of informed consent was obtained prior to data collection. Patients aged 18 years and above who were present for surgical intervention were included. All the information obtained from the patients was kept confidential and secure from unauthorised access.
Eligibility criteriaInclusion criteriaFrom June 1, 2019, to July 1, 2021, we included all adult patients aged 18 and older who underwent surgery at TGSH, as well as patients or family members who had cell phone.
Exclusion criteriaPatients who do not have cell phones are excluded.
Variables of the studyOutcome variableThe primary outcome of this study was postoperative 28-day mortality.
Independent variablesThe independent factors included sex (male/female), age (≥ 18 years), type of operation (elective or emergency), ASA physical status classification (I-V), trauma (yes/no), and comorbidity (Yes/No).
Operational definitionAnemiaDefined as Hemoglobin(Hb) less than 13 g/dl for men and 12 g/dl for non-pregnant women, and 11 g/dl for pregnant women [18].
Lost to follow-upPatients lost to follow-up within 28 days after surgery.
OutcomeThe postoperative condition of patients who survived or died within 28 days of the follow-up.
Incomplete dataMissing follow-up data due to incorrect phone numbers or inability to reach the provided phone numbers.
ComorbidityComorbidity is defined as “a distinct additional clinical entity” that exists or may emerge during the clinical course of a patient with an index disease [19, 20].
Data collection and quality controlThe data gathering methods were based on the Research Electronic Data Capture (REDCap) platform, an offline data input based on submitted questionnaires in the system [21]. The system used to collect perioperative patient information.
The anesthetist was the primary data collector at TGSH, gathering perioperative data for up to 28 days. The data manager verified that the data was complete and examined it against the hospital logbook system for inpatient mortality; if there was a discrepancy, it was cross-checked with the anesthesia and surgical logbook systems, as well as the REDCap database. After discharge, weekly follow-up phone calls were done on the 7th, 14th, 21st, and 28th postoperative days to reduce study participant dropouts. We collect multiple contact information in order to reach patients or family members. The data manager evaluated the collected data against the hospital logbook on a regular basis and filled in the gaps. The information technologist oversaw the entire REDCap database system. Prior to data collection, the anesthetist received training on the data collecting instrument as well as the ethics of recording patient data. To assure data quality, the obtained information was kept in the REDCap database system, which is only available to authorized users.
Statistical analysisData were extracted from the REDCap data server and analyzed using Stata Version 17. Categorical variables were reported as frequencies and percentages, while continuous data were tested for normality using the Kolmogorov–Smirnov test. The chi-square test was employed for categorical variables, and the T-test for normally distributed data. The variance infiltration factor (vif) was used to test for multicollinearity. The relationship between preoperative anemia and postoperative mortality was reported using an adjusted odds ratio and 95% confidence interval. Missing data were examined using the available case analysis. The propensity score match approach was used to compare anemic and non-anemic individuals. Variables included for propensity score match analysis included age, gender, comorbidities, ASA physical status, trauma, and urgency of surgery. The psmatch2 command in Stata was used for matching.
The quality of matching was assessed by balancing the variables between the anemia and non-anemia groups, and the quality of matching was tested by calculating the standardized bias before and after matching.
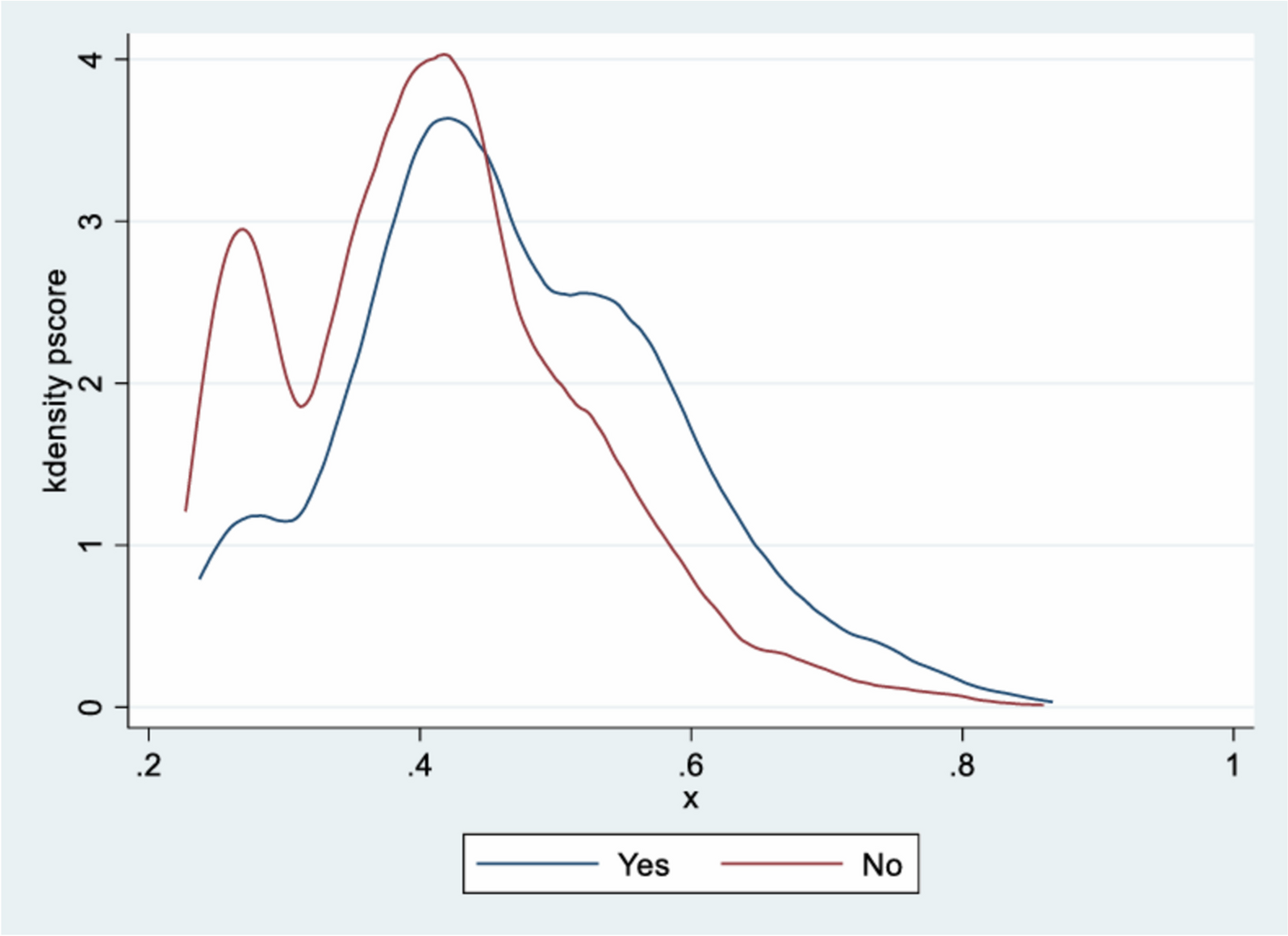
Patients with and without anemia were assigned codes 1, and 0, respectively. An adjusted estimate of the influence of preoperative anemia on postoperative 28-day mortality was produced by balancing factors classified as anemic and non-anemic based on propensity score matching. Patients with and without preoperative anemia were divided in a 1:1 ratio to balance propensity scores. To balance patients in anemic and non-anemic groups, one-to-one nearest neighbor matching was utilized with a caliber of 0.2 to estimate balancing. Standardized mean difference was used to expresses the amount of the intervention effect in each study relative to the variability found in this study. The balance of matching between anemic and non-anemic groups was also graphically assessed (Fig. 1).
Fig. 1
Assessment of matching balance in Propensity score match analysis among anemic and non anemic patients
Before and after matching, the propensity scores suggest comparable groups of anemic and non-anemic patients. The presence of preoperative anemia and its impact on surgical outcomes were assessed using an odds ratio and confidence interval. We considered balancing for statistically significant results (p-value < 0.05). A receiver operating characteristic (ROC) curve has been generated for models of preoperative hemoglobin and 28-day mortality.
留言 (0)