To the best of our knowledge, this is the first clinical trial exploring that if hyperbaric combined with hypobaric local anesthetic in subarachnoid anesthesia for cesarean section could reduce the incidence of intraoperative hypotension in pregnant women.
Cesarean section is becoming more prevalent in clinical practice, particularly with the implementation of the third-child policy in China [15]. Cesarean section procedures demand detailed attention to anesthesia and analgesia protocols. Determining the most precise and effective dosage of different specific gravity of Ropivacaine holds significant implications for ensuring the safety of both pregnant women and newborns. In this study, the efficacy of four different specific gravity of Ropivacaine in cesarean section was analyzed, providing valuable insights for future clinical medication guidance. The aim was to evaluate the outcomes resulting from the application of these doses. The objective was to furnish clinicians with a dependable reference to enhance anesthesia protocols for Cesarean section procedures.
Subarachnoid anesthesia drugs can be divided into isobaric, hypobaric and hyperbaric according to different specific gravity. If the same anesthetic is used, the dose is week, the same part is punctured, the injection speed is constant, the needle tip is oblique and the direction is facing the same side, the hyperbaric fluid flows to the low level, and the hypobaric fluid flows to the high flow, and the body position is adjusted within 10 min after injection, and a satisfactory anesthesia plane can generally be obtained. However, the isobaric is easily affected by the volume, density, and temperature of the cerebrospinal fluid, and the sensory impediment boiling plane is unpredictable [16, 17]. Compared with hyperbaric, the hypobaric has a wide range of diffusion and poor controllability [18]. Compared with the addition of 10% sugar to the hyperbaric spinal anesthesia solution, it is easier to bind to the spinal nerve, reach the required anesthesia level faster, and obtain satisfactory muscle relaxation effect, so the hyperbaric spinal anesthesia solution has become the most used spinal anesthesia drug in clinical. However, in clinical work, we have found that the weight of gravity is often caused by the high level of anesthesia, which leads to maternal hypotension [13].
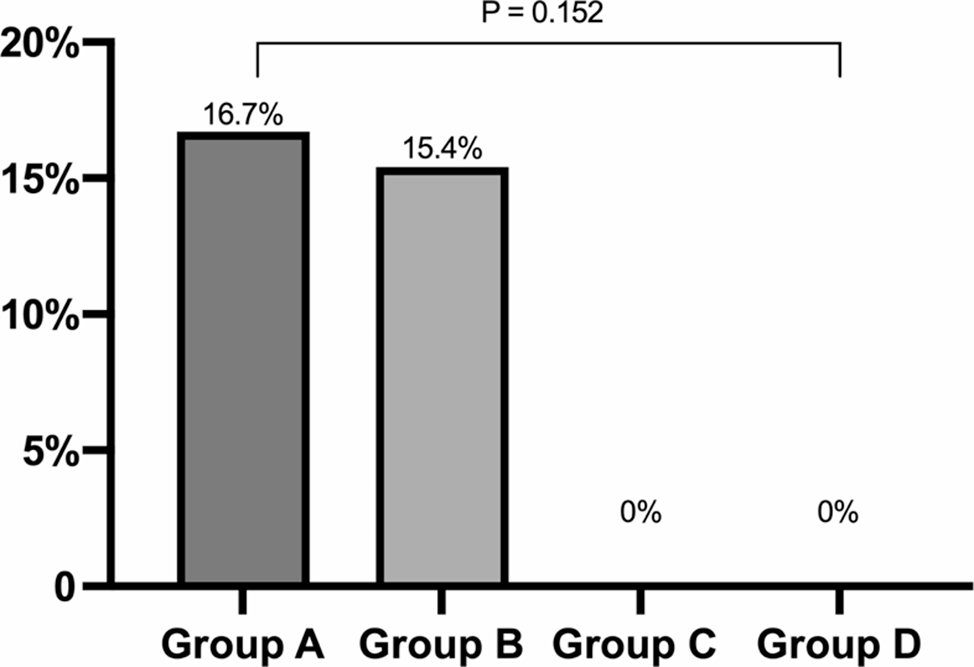
Theoretically, the method of combining hyperbaric with hypobaric, under the premise that the total dose of spinal anesthesia drug remains unchanged, can improve the cephalad movement of local anesthetic drugs, thereby reducing the occurrence of maternal hypotension during surgery. However, our results suggested that hyperbaric combined with hypobaric local anesthetic in subarachnoid anesthesia for cesarean section did not reduce the incidence of intraoperative hypotension in pregnant women. We consider that this may have something to do with the fact that our sample size was too small, as the number of hypotensive women during caesarean section was none in both group C and group D.
However, large doses of Ropivacaine have the potential to induce surgical anesthetic effects, whereas smaller doses may result in a sensory block accompanied by localized, non-progressive motor nerve block [19]. Consequently, an increase in the proportion of Ropivacaine naturally enhances its anesthetic efficacy. Analysis of the usage of additional anesthetics among the four groups revealed that the dosage administered in group A was the lowest, while that in group D was the highest, thereby reinforcing the above-mentioned observation.
In groups B, C, and D, there was a significant decrease in the rate of vasopressor utilization, indicating that reducing the proportion of Ropivacaine is more favorable for maintaining the blood pressure stability of pregnant women during caesarean section. Besides, α2-agonists seem to increase the time to first rescue analgesia and to prolong the duration of sensory block when used as adjuvants to local anesthetic in cesarean section patients. Also, α2-agonists may reduce the incidence of shivering and nausea or vomiting [20].
Tang et al. [21] also observed a lower incidence of hypotension in pregnant women following a reduction in the proportion of Ropivacaine, which aligns with our findings. We consider that this phenomenon occurs because Ropivacaine initially moves from the puncture site towards the cephalad side (from L3 to T6) when the hyperbaric anesthetic solution is administered. Subsequently, the hypobaric Ropivacaine moves from the puncture site towards the caudal side, thereby reducing the dose of local anesthetic shifting towards the cephalad side. This reduction in anesthesia level ultimately contributes to the decrease in the incidence of perioperative hypotension [22].
The increase in adverse reactions observed in group D is attributed to the low proportion of Ropivacaine, resulting in a higher concentration of anesthetic drugs migrating towards the caudal side post-injection, thus failing to achieve the desired nerve block. This hypothesis is supported by the lower satisfaction rate of abdominal wall muscle relaxation in group D compared to the other three groups.
This study also has certain limitations. First, this was a prospective cohort study and has a small sample size and the groups contribution was uneven, which night cause potential bias. Second, the trial is not international, and the participating institution of our experiment only has Nantong Maternal and Child Health Care Hospital in China. Third, only pregnant women with American Society of Anesthesiologists grades I–II were included in this trial, and those with American Society of Anesthesiologists grades III–IV were excluded. Thus, further studies including maternal women with larger sample size and randomized controlled multicenter and higher American Society of Anesthesiologists classifications are needed [23]. Improving these limitations in future research will enhance the understanding of optimal anesthesia protocols and their implications for pregnant health.



留言 (0)