
記住我



A systematic search initially identified 497 studies, of which 318 were excluded based on title and abstract review, and 35 were further excluded after full-text assessment. Fifteen studies met the inclusion criteria and were subsequently included in the meta-analysis. Among these, 6 studies focused on PFI only, 4 on RSFI only, and 5 on both. A flow diagram illustrating the study selection process is depicted in Fig. 1. Of the included studies, only three were prospective. The 11 studies addressing PFI encompassed 1535 patients and 1545 RCC lesions, while the 9 studies on RSFI involved 1617 patients and 1624 RCC lesions. In all studies, the assessment of extrarenal fat invasion was validated through histopathological analysis.
Fig. 1
Flowchart of the study selection process for the meta-analysis
Data extraction and quality assessmentThe characteristics of the studies related to extrarenal fat invasion are detailed in Tables 1 and 2, and Supplementary Tables 3 and 4, respectively. Using the QUADAS-2 tool, the assessment of the risk of bias and applicability concerns for studies on PFI and RSFI is depicted in Fig. 2a, b, respectively. For PFI studies, three studies exhibited a high risk of bias in patient selection due to nonconsecutive enrollment, case-control design, and exclusion of specific cases (patients with bilateral RCC were excluded) [11, 28, 32]; six studies had an unclear risk because they either did not specify exclusion criteria or only detailed the timing of case inclusion without confirming consecutive enrollment [13, 27, 33,34,35,36]. The risk of bias in flow and timing was high in one study due to the analysis including only a subset of patients with pathological data on PFI [36]; two studies presented an unclear risk because the time interval between CT examination and surgery was not specified [13, 34]. For RSFI, nonconsecutive enrollment primarily contributed to a high risk of bias in patient selection in one study [28]. The unclear risk of bias in four studies was due to similar reasons as those mentioned for PFI [13, 35, 37, 38]. One study excluded patients with papillary RCC and chromophobe RCC; however, since clear cell carcinoma is the predominant RCC type, the potential bias introduced by these exclusions remains uncertain. The clarity of flow and timing assessments was compromised in three studies due to unspecified time intervals [12, 13, 39], and one prospective study showed a high risk of bias because it included only a partial cohort in the analysis—some patients were either clinically unfit for surgery or were not confirmed to have RCC by pathology [38].
Table 1 The characteristics of the included studies involved the PFITable 2 The characteristics of the included studies involved the RSFIFig. 2
a Overall quality assessment of the included studies on PFI using the QUADAS-2 tool. b Overall quality assessment of the included studies on RSFI using the QUADAS-2 tool
No studies on extrarenal fat invasion were found to have a high risk of bias regarding the index test; however, one study was deemed unclear because it did not specify whether the assessment was blinded [35]. The risk of bias in the reference standard, along with applicability concerns for patient selection, index test, and reference standard, were low across all included studies.
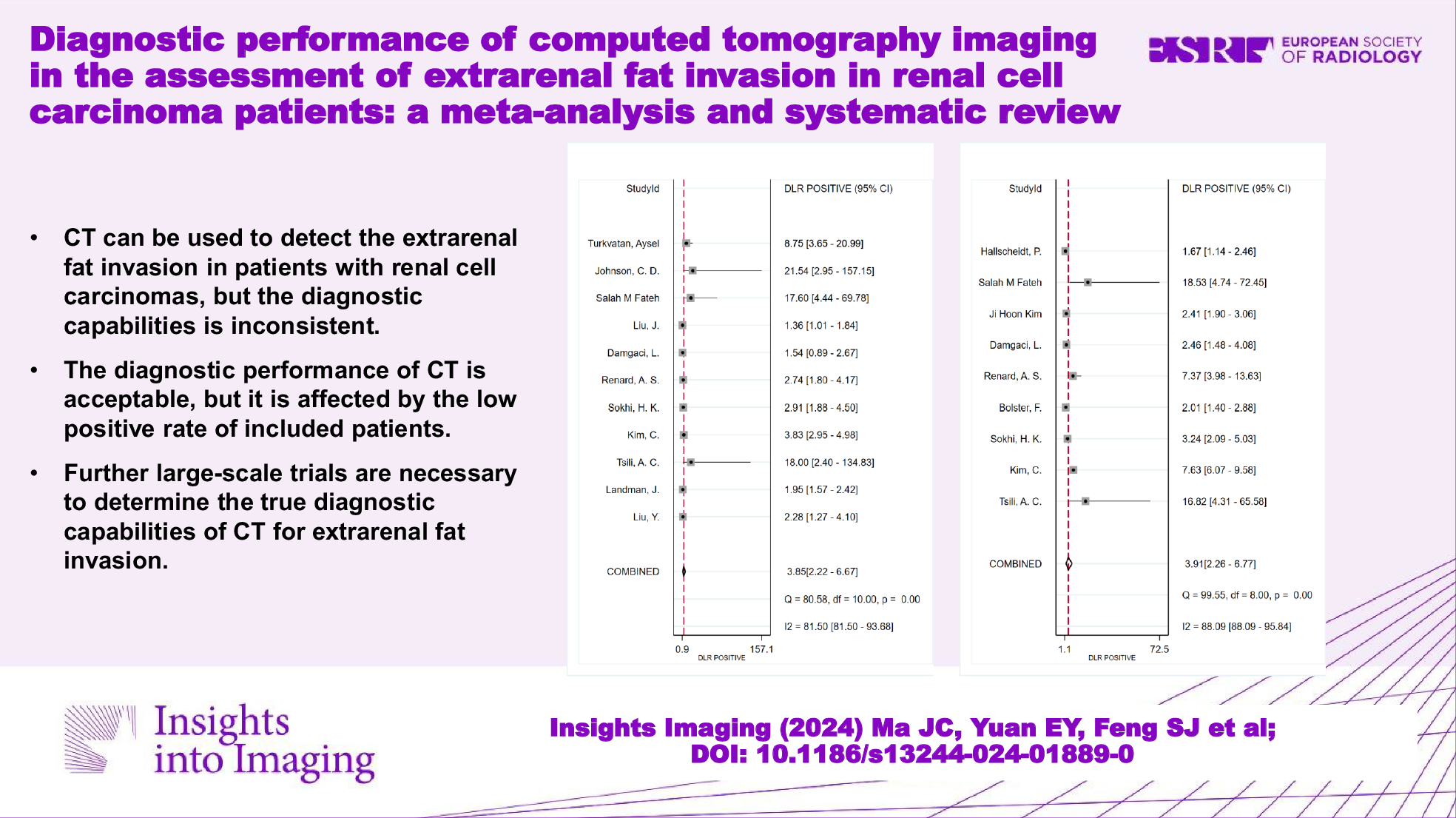
CT assessment for PFIThe sensitivity (p < 0.05, I2 = 74.11%) and specificity (p < 0.05, I2 = 92.92%) of CT assessment for PFI showed significant heterogeneity, with a pooled sensitivity of 0.69 (95% CI: 0.55–0.79) and a pooled specificity of 0.82 (95% CI: 0.69–0.90) (Fig. 3a). The combined PLR, NLR, DOR, and diagnostic score were 3.85 (95% CI: 2.22–6.67), 0.38 (95% CI: 0.27–0.55), 10.06 (95% CI: 4.82–21.00), and 2.31 (95% CI: 1.57–3.04), respectively (Fig. 3b and Supplementary Fig. 1). The area under the summary receiver operating characteristic (SROC) curve was 0.81 (95% CI: 0.77–0.84) (Fig. 3c). The accuracy parameter (Lamda) was 2.20 (95% CI: 1.46–2.95).
Fig. 3
a Forest plot of sensitivity and specificity of CT assessment for PFI. b Forest plot for likelihood ratio after combination (LR+, LR−). c The HSROC curve of CT assessment for PFI (HSROC hierarchical summary receiver operating characteristic). d The Deek funnel plot of studies on PFI
Further analysis of heterogeneity was undertaken by univariate meta-regression, which suggested that the factors influencing the diagnostic performance included the publication year and number of patients. They showed the same significant effect on specificity. The five studies published with 100 or more cases had a 70% pooled sensitivity (95% CI: 54–87; p = 0.69) and a 70% pooled specificity (95% CI: 53–98; p = 0.01). The five studies published in 2017 and later had a 76% pooled sensitivity (95% CI: 63–89; p = 0.72) and a 68% pooled specificity (95% CI: 51–86; p = 0.00). See Table 3 for detailed results.
Table 3 Results of univariate meta-regression: sources of heterogeneity involved the PFIFor imaging interpretation considering only the perinephric soft tissue density shadow-perinephric soft tissue stranding or nodules or both, the combined sensitivity, specificity, PLR, and NLR were 0.64 (95% CI: 0.40–0.83), 0.87 (95% CI: 0.70–0.95), 4.86 (95% CI: 2.27–10.44), and 0.41 (95% CI: 0.23–0.74), respectively (Supplementary Figs. 2a and 3). The area under the SROC curve was 0.83 (95% CI: 0.80–0.86) (Supplementary Fig. 2b). For imaging interpretation considering the perinephric soft tissue density shadow and other CT signs, including tumor margins, peritumoral vessels, increased density of perinephric fat et al, the combined sensitivity, specificity, PLR, and NLR were 0.72 (95% CI: 0.60–0.82), 0.74 (95% CI: 0.49–0.89), 2.74 (95% CI: 1.16–6.46), and 0.38 (95% CI: 0.21–0.67), respectively (Supplementary Figs. 2c and 4). The area under the SROC curve was 0.76 (95% CI: 0.72–0.80) (Supplementary Fig. 2d).
CT assessment for RSFIThe statistical analysis revealed significant heterogeneity in the specificity (p < 0.05, I2 = 94.05%) of CT assessments for RSFI, with pooled sensitivity at 0.81 (95% CI: 0.76–0.85) and pooled specificity at 0.79 (95% CI: 0.66–0.88), as depicted in Fig. 4a. The combined metrics of diagnostic performance, including the PLR of 3.91 (95% CI: 2.26–6.77), NLR of 0.24 (95% CI: 0.18–0.31), DOR of 16.57 (95% CI: 7.81–35.18), and diagnostic score of 2.81 (95% CI: 2.06–3.56), are illustrated in Fig. 4b and Supplementary Fig. 5. The area under the SROC curve was 0.82 (95% CI: 0.78–0.85), shown in Fig. 4c. The accuracy parameter (Lambda) was 13.30 (95% CI: −185.12 to 211.73).
Fig. 4
a Forest plot of sensitivity and specificity of CT assessment for RSFI. b Forest plot for likelihood ratio after combination (LR+, LR−). c The HSROC curve of CT assessment for RSFI. (HSROC hierarchical summary receiver operating characteristic). d The Deek funnel plot of studies on RSFI
Univariate meta-regression indicated that publication year, number of patients, number of signs, consensus read, and excretory phase significantly impacted the diagnostic performance. Among them, publication year, consensus read, and number of patients showed a significant effect on sensitivity, and the excretory phase showed a mild effect. The four studies published in 2017 and later had an 80% pooled sensitivity (95% CI: 72–87; p = 0.00) and an 82% pooled specificity (95% CI: 66–97; p = 0.87). The three studies published with consensus had an 80% pooled sensitivity (95% CI: 74–85; p = 0.00) and an 86% pooled specificity (95% CI: 73–99; p = 0.76). The three studies published with 100 or more cases had a 79% pooled sensitivity (95% CI: 73–84; p = 0.00) and an 80% pooled specificity (95% CI: 61–98; p = 0.65). The three studies published with the excretory phase had an 82% pooled sensitivity (95% CI: 75–90; p = 0.03) and a 90% pooled specificity (95% CI: 86–94; p = 0.72). Detailed results are available in Table 4.
Table 4 Results of univariate meta-regression: sources of heterogeneity involved the RSFIFor imaging interpretation considering only the signs related to renal sinus structure, the combined sensitivity, specificity, PLR, and NLR were 0.91 (95% CI: 0.79–0.96), 0.83 (95% CI: 0.57–0.95), 5.38 (95% CI: 1.81–16.05), and 0.11 (95% CI: 0.05–0.26), respectively (Supplementary Figs. 6a and 7). The area under the SROC curve was 0.92 (95% CI: 0.90–0.94) (Supplementary Fig. 6b). For imaging interpretation considering the other signs (not related to renal sinus structure), the combined sensitivity, specificity, PLR, and NLR were 0.79 (95% CI: 0.71–0.85), 0.72 (95% CI: 0.55–0.84), 2.81 (95% CI: 1.60–4.93), and 0.29 (95% CI: 0.19–0.45), respectively (Supplementary Figs. 6c and 8). The area under the SROC curve was 0.81 (95% CI: 0.77–0.84) (Supplementary Fig. 6d).
Publication biasThe Deek’s funnel plot of studies on PFI and RSFI showed a slope coefficient of 0.03 and 0.64, respectively, which indicate that there was mild publication bias in the included studies on PFI and no publication bias in the included studies on RSFI (Figs. 3d and 4d).
留言 (0)