
記住我



The final study population consisted of 37 patients (20 male, 17 female). Median age was 56 years (IQR, 19 years; range, 19–88 years) who underwent CCTA after intravenous injection of landiolol hydrochloride due to a heart rate > 60 bpm. Median body weight was 77 kg (IQR, 32 kg; range, 50–130 kg), median body height was 172 cm (IQR, 12 cm; range, 150–190 cm), and median body mass index was 25 kg/m² (IQR, 7 kg/m²; range, 17–44 kg/m²). Fourteen patients received oral beta-blocker 1 h before the examination (Bisoprolol 1.25 mg in one patient, Bisoprolol 2.5 mg in five patients, Bisoprolol 5 mg in four patients, Bisoprolol 10 mg in one patient, Carvedilol 12.5 mg in one patient, Carvedilol 25 mg in one patient, and Nebivolol 2.5 mg in one patient), whereas in 23 patients no oral beta-blocker was administered by the referring physicians. 0.4 mg Glyceroltrinitrat was administered in 32 patients, in five patients glyceroltrinitrat was withhold due to lack of sufficient information on contraindication at the time point of examination at the Radiology.
Cardiac ultrasound was performed in 34/37 patients within 2 weeks to CCTA. Ejection fraction was normal in 29 patients (78.4%), moderately reduced in four patients (10.8%), and reduced in one patient (2.7%). In three patients (8.1%), no cardiac ultrasound within 2 weeks of CCTA was available.
All 37 individuals enrolled in the study received the study drug; however, only 15 patients received all six partial injections (a maximum amount of 60 mg) of landiolol hydrochloride. Given that the required heart rate (≤ 60 bpm) of the remaining 22 patients was received without using the maximum study dose of landiolol hydrochloride, the application of the remaining partial doses was relinquished. Three patients received one dose (7 mg), twelve patients received two doses (20 mg), no patient received three doses, seven patients received four doses (40 mg) and no patient received five doses. The mean dose (± SD) was 0.526 ± 0.3 mg/kg (95% CI, 0.426–0.626 mg/kg). No adverse effects occurred after landiolol hydrochloride administration in our patient cohort.
Image quality of the CCTA was categorized as excellent (no, to almost no motion artifacts) in 21 patients, good (minor motion artifacts without relevant influence on image interpretation) in 10 patients, moderate (some motion artifacts with little influence on image interpretation) in 5 patients, and poor (substantial motion artifacts with important influence on image interpretation) in 1 patient.
In 19 patients (51.4%), CCTA was reported as CAD-RADS 0, in 8 patients (21.6%) as CAD-RADS 1, in 1 patient (2.7%) as CAD-RADS 2, in 3 patients (8.1%) as CAD-RADS 3, in 4 patients (10.8%) as CAD-RADS 4a, and in 1 patient (2.7%) as CAD-RADS 4b. In 1 patient (2.7%), the CCTA study was non-diagnostic (CAD-RADS N).
Tables 1 and 2 show details on HR before landiolol hydrochloride injection, during using our scheme of fractional landiolol hydrochloride administration, during CCTA and after the CT examination as well as BP before and after CCTA. A statistically significant decrease of HR by −12 bpm during fractional landiolol hydrochloride administration compared to the initial HR was observed. We also found a statistically significant increase of HR by +2 bpm during CCTA compared to the lowest HR during fractional landiolol hydrochloride administration. Despite the increase of HR during CCTA compared to the HR during fractional landiolol hydrochloride administration, there was still a statistically significant reduction of HR by −9 bpm compared to the initial HR before landiolol hydrochloride injection.
Table 1 Heart rate before landiolol hydrochloride administration (HRPRE), heart rate after last partial landiolol hydrochloride injection (HR1–6), heart rate during cardiac CT (HRCT) and heart rate after cardiac CT (HRPOST), as well as blood pressure (BPSYST, BPDIAST) before and after cardiac CT (n = 37)Table 2 Change in heart rate (HR) and blood pressure (BPSYST and BPDIAST) after landiolol hydrochloride injection (n = 37)During fractional landiolol hydrochloride administration, a HR ≤ 60 bpm was achieved in 22 patients (60%) and a HR of ≥ 60 bpm, but ≤ 65 bpm was achieved in 6 patients.
During CCTA, a HR ≤ 60 bpm occurred in 13 patients (35%) and a HR of ≥ 60 bpm, but ≤ 65 occurred in 12 patients. So overall, during fractional landiolol hydrochloride administration, a HR of ≤ 65 bpm was achieved in 28 patients (76%) and during CCTA, a HR of ≤ 65 bpm was achieved in 25 patients (68%).
Although a statistically significant smaller decrease of HR after landiolol hydrochloride injection occurred in patients with oral beta-blocker premedication than in patients without prior oral medication, the difference between the HR during CCTA and the initial HR was also statistically significant in this subgroup (Table 2).
In patients who additionally received glyceroltrinitrat, statistically significant lower blood pressure was measured after the CT examination compared to the initial blood pressure. On the contrary, no statistically significant change in blood pressure was seen in patients with landiolol hydrochloride medication only (Table 2).
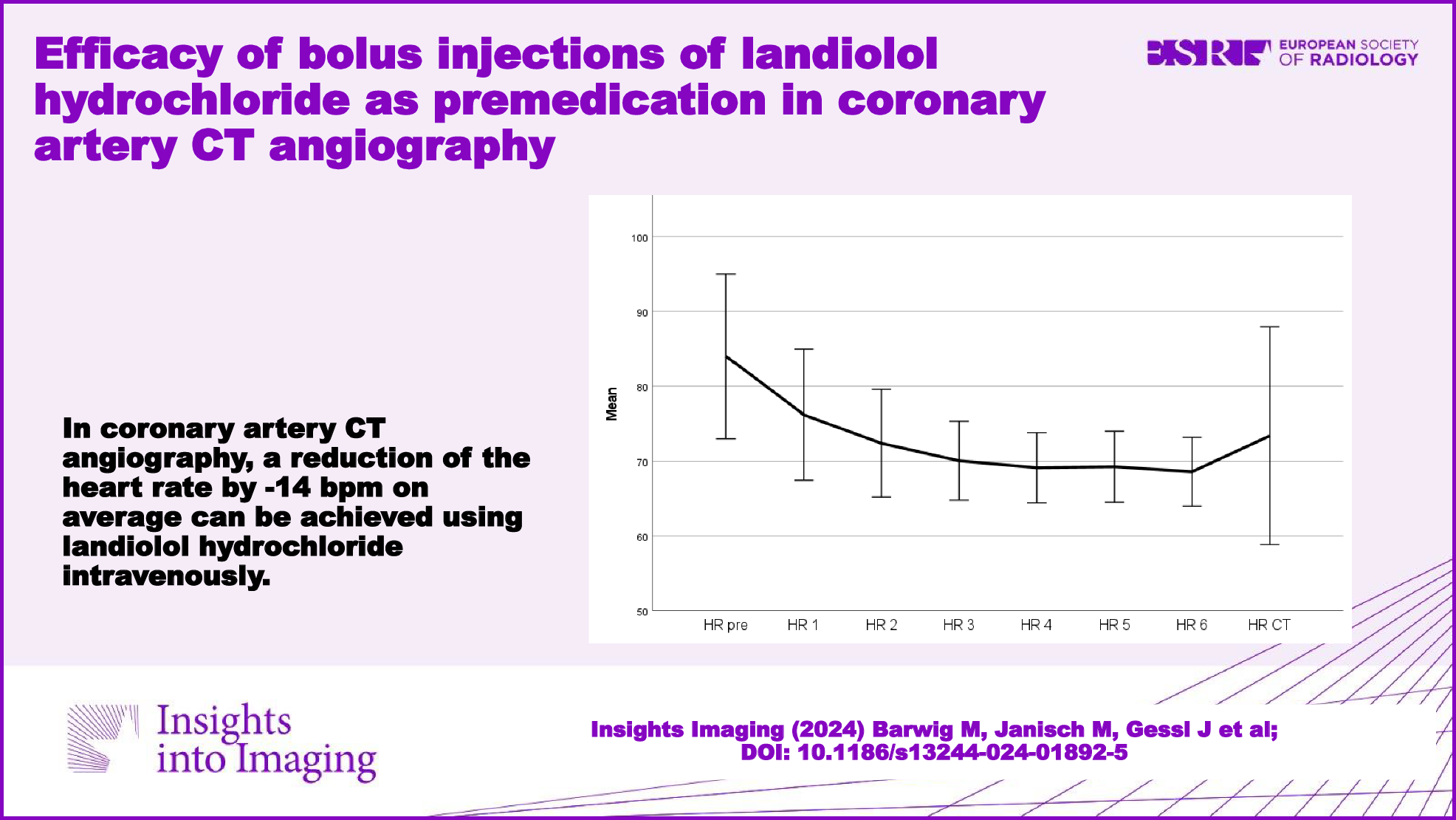
In patients who received the full dose (60 mg) of landiolol hydrochloride according to our study protocol (n = 15), each partial injection up to the fourth injection led to a statistically significant decrease in the HR compared to the HR after the previous injection. The fifth and sixth injections did not result in a further statistically significant decrease of the HR (Table 3). Figure 2 visualizes the course of the mean HR after the application of each partial dose. A clear reduction of the HR after injection of the first three doses of landiolol hydrochloride was observed. A less distinct, yet significant decrease of the HR after the fourth injection was achieved. However, after the fifth partial injection of landiolol hydrochloride no significant change of the HR was detectable.
Table 3 Heart rate before landiolol hydrochloride administration (HRPRE) and after each partial injections (HR1–HR6) in individuals who received all six injections of landiolol hydrochloride (n = 15)Fig. 2
Mean HR and standard deviation after stepwise application of landiolol hydrochloride and during cardiac CT in patients who received the full dose of 60 mg in six injections (15 patients)
HR decrease following landiolol hydrochloride injection was not influenced by sex (p = 0.258), body height (p = 0.254), body weight (p = 0.285) or body mass index (p = 0.180), indicating that the injection schema used in this study compensated for a possible influence of these allometric parameters on landiolol hydrochloride effectiveness.
留言 (0)