
記住我



A total of 249 patients (126 male, 123 female) with a mean age of 50.0 ± 12.9 years (range, 19–78 years) were included. The mean body mass index (BMI) was 22.9 ± 3.0 kg/m2 (range, 12.5–32.6 kg/m2), with 16 patients with BMI < 18.5 kg/m2 and 91 patients with BMI ≥ 24 kg/m2. Patient characteristics are summarized in Table 2.
Table 2 Patient characteristicsAccording to the reference standard, a total of 637 lung nodules were identified. Among them, 368 (57.8%) were solid, 35 (5.5%) were part-solid, and 234 (36.7%) were pure ground-glass. The nodules were divided according to the type (solid, part-solid, and pure ground-glass) and Lung-RADS category for subgroup analysis.
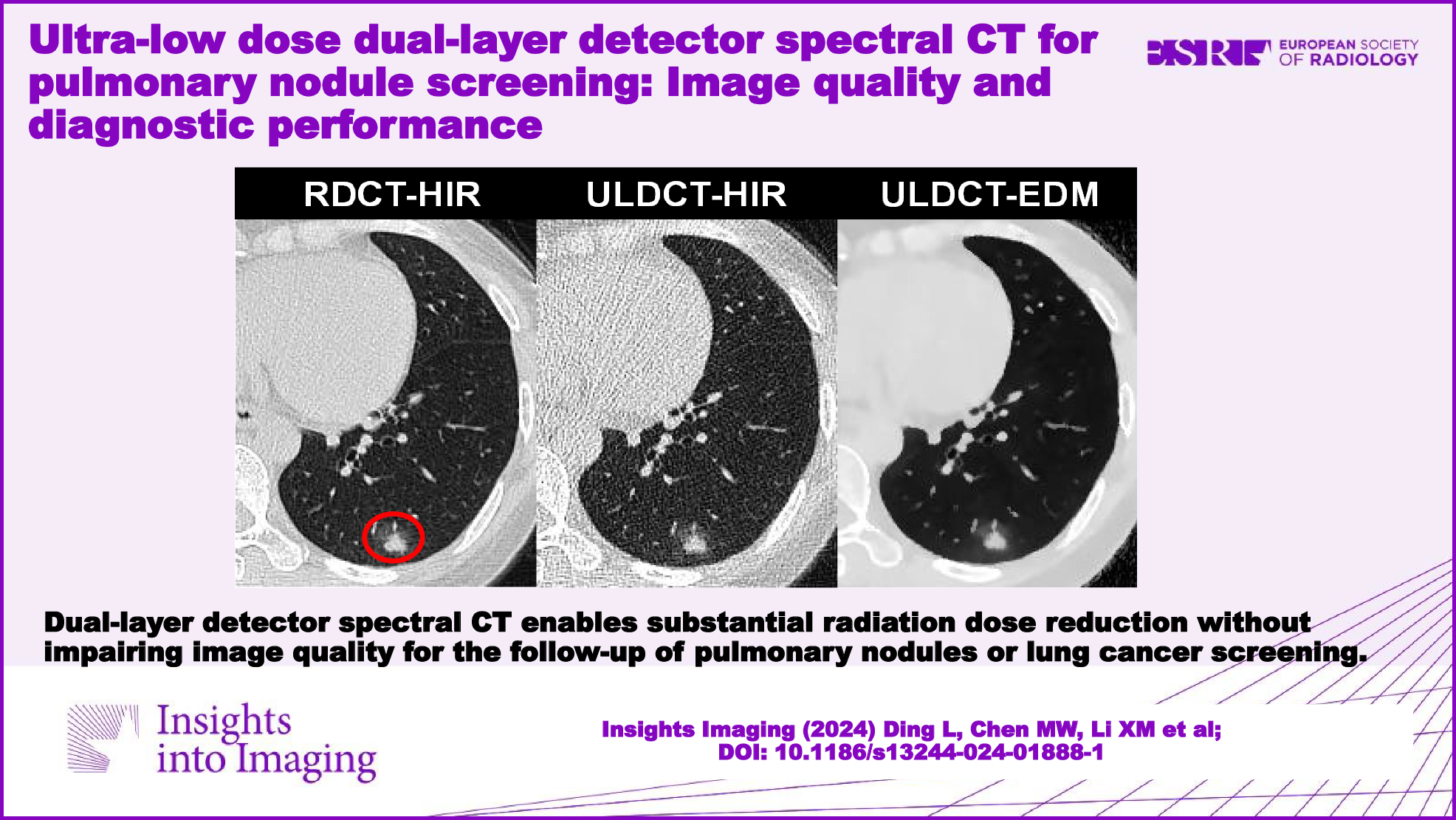
Radiation doseThe mean CTDIvol (0.5 mGy × cm ± 0.0 vs. 5.6 ± 1.2 mGy × cm; p < 0.001) and dose-length product (23.0 mGy ×cm ± 1.4 vs. 258.4 mGy × cm ± 54.4; p < 0.001) were significantly lower with ULDCT than with RDCT. The mean effective dose of RDCT and ULDCT was 3.6 mSv ± 0.8 and 0.3 mSv ± 0.0, respectively, indicating a significant dose reduction of 91.2% (p < .001).
Qualitative image analysisFigure 2 shows box plots of the qualitative scoring results. For ULDCT images, all image quality parameters were ranked superior with EDM when compared with HIR and VMIs (p < 0.05 for all comparisons). Notably, the average scores of ULDCT EDM in each assessment item were higher or equal to the average (score 3 on a 5-point scale). The inter-observer agreement (kappa value) for streak artifact, image noise, clarity of small vessels, visibility of nodules, and the overall image quality were 0.75, 0.70, 0.71, 0.74, and 0.68, respectively.
Fig. 2
The box plots show the qualitative image quality scoring results. For visibility of pulmonary nodules, no statistically significant difference is found between RDCT HIR and ULDCT EDM (p > 0.05). And significant differences are observed among other reconstruction groups (p < 0.001 for all). DLSCT, dual-layer detector spectral CT; RDCT, regular-dose CT; ULDCT, ultra-low dose CT; HIR, hybrid iterative reconstruction; VMI, virtual monoenergetic image; EDM, electron density mapping
In detail, overall image quality for ULDCT EDM was rated as excellent in 15.5% (99 of 637), good in 48.8% (311 of 637), and moderate in 34.2% (218 of 637). In terms of the visibility of all pulmonary nodules, the difference was not significant between RDCT HIR and ULDCT EDM (4.4 ± 0.8 vs. 4.3 ± 0.8; p > 0.05). For pure GGN, ULDCT EDM scored significantly better than RDCT HIR (4.0 ± 0.8 vs. 3.6 ± 0.7; p < 0.001). For part-solid nodules, a similar result was found (ULDCT EDM 4.8 ± 0.4 vs. RDCT HIR 4.7 ± 0.6, p > 0.05). For solid nodules, RDCT HIR achieved the highest score (4.5 ± 0.7), and EDM and VMI40 keV on ULDCT were of diagnostic quality (score > 3). Examples of RDCT and ULDCT images in participants were provided in Figs. 3–5. Detailed qualitative analysis results were provided in the Supplementary Materials (Appendix E2).
Fig. 3
DLSCT at different radiation doses and reconstruction algorithms in a 65-year-old female (BMI: 21.2 kg/m2) with a solid nodule in the right lower lobe (circle). RDCT, regular-dose CT; ULDCT, ultra-low dose CT; HIR, hybrid iterative reconstruction; VMI, virtual monoenergetic image; EDM, electron density mapping
Fig. 4
DLSCT at different radiation doses and reconstruction algorithms in a 49-year-old female (BMI: 19.5 kg/m2) with a part-solid nodule in the left lower lobe (circle). RDCT, regular-dose CT; ULDCT, ultra-low dose CT; HIR, hybrid iterative reconstruction; VMI, virtual monoenergetic image; EDM, electron density mapping
Fig. 5
DLSCT at different radiation doses and reconstruction algorithms in a 67-year-old male (BMI: 25.4 kg/m2) with a pure ground-glass nodule in the right upper lobe (circle). RDCT, regular-dose CT; ULDCT, ultra-low dose CT; HIR, hybrid iterative reconstruction; VMI, virtual monoenergetic image; EDM, electron density mapping
Quantitative image analysisQuantitative assessment results are summarized in Table 3. There were significant differences in CT numbers among different groups (all p < 0.001). ULDCT EDM revealed significantly lower noise in fat, aorta, and muscle than other reconstructions (p < 0.001 for all comparisons). Compared with RDCT HIR, ULDCT EDM showed significantly higher SNR (44.0 ± 77.2 vs. 4.6 ± 6.6; p < 0.001) and CNR (26.7 ± 17.7 vs. 5.0 ± 4.4; p < 0.001) for pulmonary nodules. Furthermore, VMIs at 40 keV and 70 keV of ULDCT yielded lower noise and higher SNR than ULDCT HIR, although the differences were not statistically significant (p > 0.05 for all).
Table 3 Quantitative image quality analysis resultsDiagnostic performanceNodule detection rates were given in Table 4, categorized by nodule type, reconstructions, and Lung-RADS category. Compared with the reference standard, reconstruction techniques of ULDCT images performed good detection of solid nodules, with a similar nodule detection rate (78.3%–82.6%). Among all reconstructions, only 1 of 35 part-solid nodules, sizing 10 mm, was missed on VMI70keV. For pure GGNs, EDM showed a significantly higher nodule detection rate (85.5%, 200/234), compared with HIR (76.9%, 180/234), VMI40keV (76.5%, 179/234), and VMI70keV (71.8%, 168/234). On EDM, 34 pure GGNs not identified, and all of them were less-than 6 mm in diameter.
Table 4 The nodule detection rates at ULDCT according to the reference standardThe results of inter-scan agreement and inter-observer agreement were summarized in Table 5. Inter-scan agreements between ULDCT and SDCT were good (all κw > 0.60, both reader 1 and reader 2). The inter-observer agreements between the two readers were good for ULDCT HIR and ULDCT VMI70keV, and excellent for ULDCT EDM and ULDCT VMI40keV.
Table 5 Inter-scan and Inter-observer agreement for Lung-RADS resultsThe consistency of measurement between RDCT and ULDCT was excellent for diameter ((ICC value) RDCT vs. ULDCT HIR: 0.907, RDCT vs. ULDCT EDM: 0.913, RDCT vs. ULDCT VMI40keV: 0.901, RDCT vs. ULDCT VMI70keV: 0.895) and volume ((ICC value) RDCT vs. ULDCT HIR: 0.977, RDCT vs. ULDCT EDM: 0.989, RDCT vs. ULDCT VMI40keV: 0.981, RDCT vs. ULDCT VMI70keV: 0.975). Consistency in nodule diameter and volume measurements between the two readers was excellent (all ICC values > 0.80). Figure 6 shows the Bland-Altman plots of RDCT HIR vs. ULDCT EDM for diameter and volume measurements. Subgroup analysis based on nodule type and size is provided in the Supplementary Materials (Appendix E3).
Fig. 6
Bland-Altman plots show the consistency of diameter measurement (a) and volume measurement (b) between RDCT HIR and ULDCT EDM. RDCT, regular-dose CT; ULDCT, ultra-low dose CT; HIR, hybrid iterative reconstruction; EDM, electron density mapping
留言 (0)