Summary
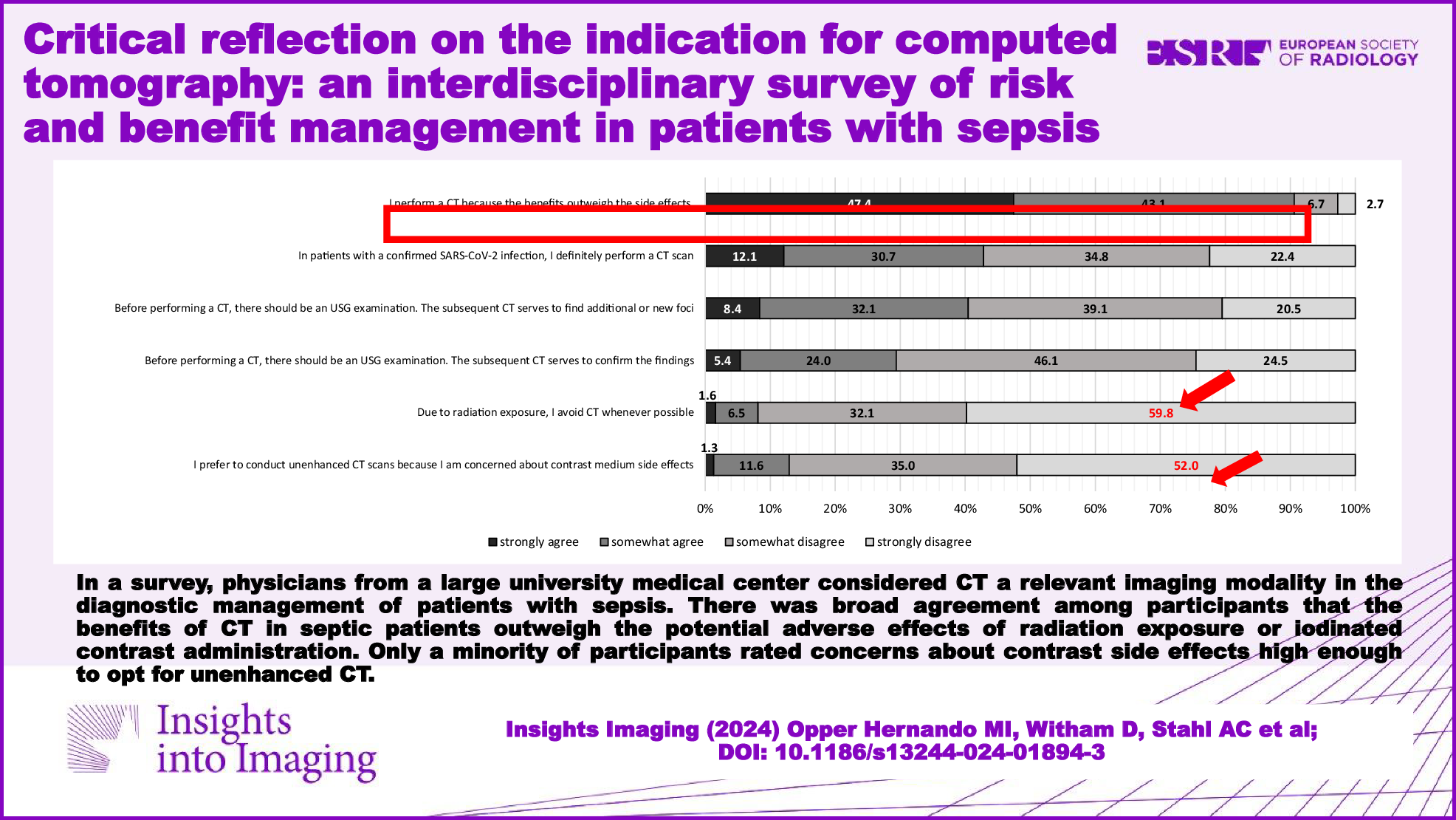
There is agreement among the participants of our questionnaire survey that the benefits of a CT scan in septic patients are greater than the potential adverse effects of radiation exposure or ICM administration. They see the strongest indication for a CECT when searching for an infectious focus in the abdomen alone or simultaneously in the abdomen, chest, and pelvis regions. A history of a severe allergic reaction after contrast administration was considered a relative to absolute contraindication. However, in patients with a history of mild adverse effects or manifest hyperthyroidism, respondents generally favored the option of specific preparation prior to CECT. If an initial CT scan cannot detect a source of infection, doctors recognize alternative and/or accompanying diagnostic tools as an essential part of managing sepsis. At the same time, the participants perceived repeated CT scans as a good option for septic patients with clinical deterioration.
Literature
To our knowledge, this is the first study to explore physicians’ perspectives on the use of CT in patients with sepsis, with no other literature available on this topic aside from our previous work [18]. Despite exposure to ionizing radiation, imaging remains a crucial component of clinical practice for diagnosing various conditions [8, 13, 15]. Advances in technology and adherence to the ALARA (as low as reasonably achievable) principle have constantly reduced the risks associated with ionizing radiation over recent decades [13, 25, 26]. Nevertheless, any CT examination must be justified, meaning the benefits should outweigh the risks [14, 27]. The sepsis guidelines emphasize the rapid search for foci of infection but do not explicitly state that sepsis justifies a CT indication [5, 6]. The participants of our survey regard the prompt identification of an infection source in septic patients as a justified indication for a CT scan and the associated radiation exposure. However, participants’ caution is evident in their reluctance to perform repeat CT scans after 3 days in clinically unaltered or follow-up scans after 1 week in clinically improved septic patients, demonstrating their intent to minimize unnecessary radiation exposure.
The use of contrast media is necessary for certain CT examinations and has been shown to improve diagnostic accuracy [14, 28]. In guidelines for the general use of CT, CECT is explicitly recommended for the assessment of abdominal and soft tissue infections [12, 14, 28, 29]. Consistent with these guideline recommendations, our participants identified the strongest indication for a CECT when examining the abdomen or a combined examination of the chest, abdomen, and pelvis. In our survey, there was agreement between experienced physicians and radiologists that infectious foci in the abdominal cavity are challenging to detect on unenhanced CT scans.
Before administering ICM, the patient’s individual risk of adverse reactions should be assessed [29,30,31]. Given that the literature describes mild adverse reactions as typically self-limiting [19, 31], participants considered the use of CECT with premedication to be appropriate. Still, the majority of physicians (43.1%) considered a history of severe adverse reactions to ICM as an absolute contraindication for CECT in septic patients. Interestingly, we have shown before that 75% of final-year medical students judge this as an absolute contraindication [24]. Similarly, Alchallah et al found that 65.4% of medical students saw a severe allergic reaction as an absolute contraindication [32]. Fortunately, the risk of moderate to severe adverse events has decreased in recent decades (incidence < 0.04%), largely due to the development of safer ICMs [19, 30, 31]. Nonetheless, we must be aware that severe adverse reactions can cause life-threatening conditions [19, 31].
Another concern in clinical practice is the development of acute renal failure due to the administration of ICM, known as CIN. In accordance with the literature, our participants considered ICM administration rather safe in patients with end-stage renal failure requiring dialysis [19]. However, in less progressed chronic kidney disease (CKD) with residual kidney function, a higher risk of developing CIN has been discussed [19, 20, 33]. Consistent with this, physicians expressed concern about ICM use in septic patients with a creatinine level > 2 mg/dL or eGFR < 30 mL/min. Currently, premedication and other prophylactic measures, such as appropriate hydration, are suggested for patients with CKD and an eGFR < 30 mL/min [19, 20, 29, 31, 34]. The incidence of CIN ranges from around 2% in the general population to around 30% in patients at a high risk of developing kidney disease [19, 35]. Davenport et al argue that the risk of AKI associated with ICM administration has been overstated [34]. Accordingly, Tong et al reported no statistically significant increase in the risk of CIN among patients undergoing CECT compared to those examined by unenhanced CT [36]. The findings of Hsu et al show no increased risk of AKI in septic patients undergoing CECT, highlighting AKI as a potential complication of sepsis [37].
Physicians participating in our survey were aware of the risks associated with ICM administration in patients with hyperthyroidism. The European Society of Emergency Radiology and the European Thyroid Association list hyperthyroidism as a contraindication to the administration of ICM [31, 38]. However, in emergency situations where CECT is necessary, Bednarczuk et al state that even patients with manifest hyperthyroidism can undergo the scan with premedication as a preventive measure [38]. Consistent with this, most participants favored premedication over a uniform rejection of CECT in septic patients with hyperthyroidism. While there is no literature on the preferred choices of different medical specialties, our participating radiologists stood out as being more skeptical of using ICM in patients with manifest hyperthyroidism compared to other specialties.
Overall, most published studies and guidelines on the use of CT or contrast media do not specifically address septic patients. The question that remains is whether sepsis should be considered an extreme emergency, possibly warranting less focus on the risks and adverse effects of CT and ICM in clinical decision-making, or whether potential adverse events pose an even greater risk to septic patients.
Limitations
Even though only a minority of physicians surveyed responded, i.e., approximately 15%, this response rate can be deemed sufficient for providing an overview of physicians’ perspectives on the survey’s topic. Our center comprises three university hospitals, offering a diverse and substantial patient population as well as varied perspectives from healthcare professionals. This setup allowed us to generate robust data and meaningful insights within a single-center framework. While our data reflect the viewpoints of physicians from different settings involved in the management of sepsis, these findings may not accurately represent physicians’ perspectives from different healthcare facilities or different countries. However, our results reflect the heterogeneous variety of work experiences, workplaces, and physicians’ medical specialties in managing septic patients. Lastly, our survey used closed-ended questions with a limited number of options instead of open-ended questions. Therefore, we decided to use 4-point scales instead of 5-point scales to at least avoid the limitation of participants’ tendency to choose the middle of the response spectrum on a Likert scale.
Conclusion
Physicians across different specialties, workplaces, and work experience levels view CT as a diagnostic pillar for managing patients with sepsis. However, detailed research is needed to assess the risks associated with contrast media and the diagnostic value of CECT in identifying infectious foci in septic patients. Future studies should aim at generating better evidence on the use of CT in septic patients to achieve the best outcome.




留言 (0)