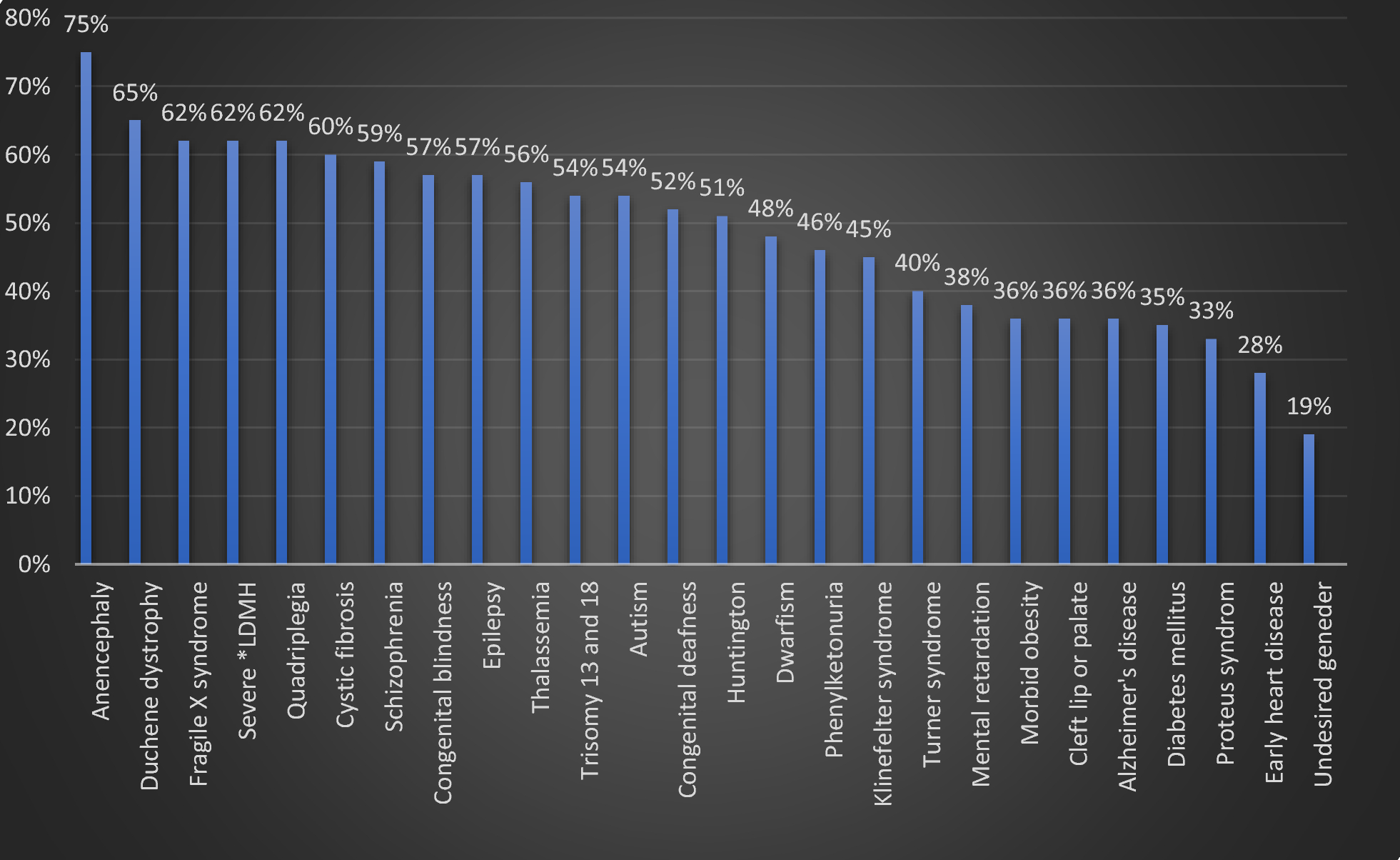
The current study evaluated the rate of abortion decisions and associated factors among pregnant women in Mashhad, Iran, in the case of genetic disorders or undesired gender in their unborn child. Mashhad is one of the most populated cities in Iran. Also, it is the biggest city and the main clinical referral center in northeastern Iran; therefore, the present study can be attributable to the northeastern population of Iran. Among genetic disorders, the highest rate of abortion agreement referred to anencephaly (75%), and the lowest one referred to early heart disease (28%). Also, the rate of abortion agreement was equal with 19% toward undesired baby's gender, which was lower than all genetic disorders. The present study showed that various demographic factors are associated with abortion agreements. Education was associated with abortion agreement in cleft lip or palate, Alzheimer's disease, Turner syndrome, CF, PKU, Huntington, autism, fragile X syndrome, and epilepsy. The number of children was correlated to abortion agreement in congenital blindness, DMD, autism, Proteus syndrome, Klinefelter syndrome, anencephaly, MR, quadriplegia, and severe LDMH. Age was associated with abortion agreement in conditions such as epilepsy, congenital blindness, schizophrenia, and severe LDMH. History of an anomaly in previous pregnancies could be related to abortion decisions in Klinefelter syndrome, Turner syndrome, dwarfism, and quadriplegia. The number of pregnancies was associated with abortion decisions in severe LDMH, dwarfism, and Klinefelter syndrome. Job status was correlated to abortion decisions in epilepsy, Alzheimer's disease, and dwarfism. Congenital abnormalities are significantly prevalent in Iran (38.3/1000), including congenital deformities (17.9/1000), single gene disorders (16.4/1000 with G6PD), chromosomal abnormalities (3.1/1000), and congenital infections (0.9/1000). Of these, musculoskeletal disorders, dermatologic manifestations, and urogenital deformities were more prevalent. However, their distribution is variable regarding ethnicities because of socioeconomic status, genetic variations, and the rate of consanguineous marriages [11]. The rate of consanguineous marriage is notably high in Iran (38.6%), which accounts for the high prevalence of genetic disorders [5]. Prenatal testing for the detection of genetic disorders has progressed significantly around the world during the last decades [12]. One of the successful Iranian prenatal care programs, called the “thalassemia program,” was conducted in 1997. Until 2001, more than 2.7 million couples were screened, and 10,298 at-risk couples were detected. Genetic counseling for these couples was responsible for a 70% decrease in the annual birth rate of infants with thalassemia [8]. According to prenatal diagnosis (PND), legal abortion is permitted in Iran before the 16th gestational week if the diagnosis is confirmed [6]. Abolghasemi et al. evaluated the plan of thalassemia prevention in Iran. During PND, 2819 couples (2549 fetuses) were tested, and 98% of couples agreed to terminate the pregnancy after thalassemia had been diagnosed in their fetuses. The remaining 2% did not perform abortions due to late referral to PND centers, cultural matters, and multiple pregnancies, with various results for each [13]. Similarly, our study showed that the number of children is not associated with abortion decisions for a child with thalassemia. The other demographic factors were not associated with abortion decisions in thalassemia, too. Hamzehloei et al. investigated the frequency and type of thalassemia mutations in northeast Iran. They concluded that thalassemia mutations in this region differ from those in other parts of Iran. This point highlights that genetic counseling and prenatal testing should be optimized based on the region and type of mutations [14]. Wyszynski et al. evaluated the rate of abortion agreement among 165 parents with a child suffering from non-syndromic oral clefts in Argentina. None of them agreed with the termination of pregnancy if their unborn child had this disorder again, but only 6.1% would terminate the pregnancy in the case of Down syndrome in addition to the oral cleft [15]. Our study presented that 36% of pregnant women would decide to terminate their pregnancy if their child had a cleft lip or palate. Among demographic factors, only the level of education was associated with this decision. Quadrelli et al. studied parental decisions to terminate or continue a pregnancy regarding abnormalities and aneuploidies of somatic and sex chromosomes in Uruguay. Among 207 couples, 89% and 96% of patients chose to terminate their pregnancy, facing Down syndrome and aneuploidy with poor prognosis, respectively. When challenged with sex chromosomal aneuploidy or aneuploidies with a minimal chance of an aberrant clinical phenotype, 79% and 90% of individuals decided to continue the pregnancy, respectively. Also, they found that only maternal age is correlated to decision-making of pregnancy in Down syndrome [16]. We found that the intention of abortion is about 40%-60% in chromosomal aneuploidies, including trisomy 13/18, Klinefelter syndrome, and Turner syndrome. In these disorders, demographic factors such as a history of previous anomalies were associated with abortion agreement in Klinefelter syndrome and Turner syndrome. The education level was associated with abortion agreement in Turner syndrome. Also, the Abortion decision facing Klinefelter syndrome was correlated to the number of pregnancies and children. Shaffer et al. analyzed pregnancy termination rates for different fetal aneuploidies among 833 American women and assessed the determinants of this decision. Similarly, the rate of abortion decisions was higher in trisomy 13/18 compared to Turner and Klinefelter syndromes. Also, they found that maternal age, ethnicity, aneuploidy severity, and kind of diagnostic method are correlated to abortion decisions faced with aneuploidies [17]. A cohort study conducted in Denmark detected 320 fetuses with abnormalities. Of these, 67% of these families were informed about the termination of pregnancy, and 92% of them agreed to abort their child. The intention of ending or continuing a pregnancy was linked to first-trimester diagnoses, singleton pregnancies, fatal illnesses, and genetic disorders. Adjusting for the diagnosis time showed that the only significant factor for determining an abortion decision referred to the fatal prognosis. In this cohort, the fatal prognosis included holoprosencephaly, anencephaly, and bilateral renal agenesis [18]. According to the present study, the most prevalent cause of abortion decisions was the presence of anencephaly in future children (75%). Zlotogora evaluated 1467 women who performed invasive PND testing, and fetus abnormality was confirmed. These women were categorized into two groups, including Jews and Muslims. Most Muslim women decide to terminate their pregnancy based on the severity of detected genetic disorders in their child, except in hemoglobinopathies and a group of significant chromosomal abnormalities. The author hypothesized that this exception could be attributable to their religious beliefs. Also, he concluded that the severity of genetic disorders is the main factor for deciding about pregnancy termination, while the time of diagnosis could be necessary among Muslims [19]. Saudi Arabia is a Muslim country with a high rate of consanguineous marriages, similar to Iran. However, there are significant distinctions in culture and religious denomination. AbdulAzeez et al. evaluated 2761 Saudis toward abortion decisions and PND. They concluded that education, history of genetic disorders in previous pregnancies, consanguinity, history of abortion, and religion were the determinant factors in the termination of pregnancy among Saudi participants, and religious beliefs were the most crucial factor [20].
As in previous studies, our findings confirmed that decision-making regarding pregnancy termination can be variable region by region. Considering our limitations, studying a larger sample representing different ethnicities and religions, as well as longitudinal follow-up, is crucial in future studies.





留言 (0)