
記住我
A total of 84 patients were included in this study, comprising 35 individuals with video PSG-confirmed iRBD, 29 with PD, and 20 with DLB patients. We categorized the participants into three groups according to the cognitive status; 19 LBD-Cognitively Normal (LBD-CN), 45 LBD-Mild Cognitive Impairment (LBD-MCI), and 20 Lewy body dementia. With the exception of age, there were no statistically significant differences among the three groups in terms of sex, years of education, or the duration of RBD, PD, or DLB. The detailed demographics and clinical features are presented in Table 1. Significant differences were observed among the three groups in MDS-UPDRS parts 1, 2, and 3, as well as in the total score. Moreover, these scores exhibited an increasing trend from CN to MCI, and then to dementia group (p < 0.001). Among the subdomains of the MDS-UPDRS part 1, we observed significant differences in hallucinations and psychosis (part 1.2, p = 0.001), depressed mood (part 1.3, p = 0.019), anxious mood (part 1.4, p = 0.001), and apathy (part 1.5, p = 0.014) scores across the three groups, even after adjusting for age. Additionally, there was an increasing trend in these subdomain scores from CN to MCI, and then to dementia groups. Neuropsychological tests demonstrated that the MCI and dementia group performed significantly worse than the CN group in attention (TMT-A; p = 0.004), language (K-BNT; p < 0.001), memory (RCFT delayed recall; p = 0.017), and frontal/executive functions (COWAT phonemic; p < 0.001, K-CWST color reading; p < 0.001, DSC; p = 0.012, TMT-B; p = 0.007).
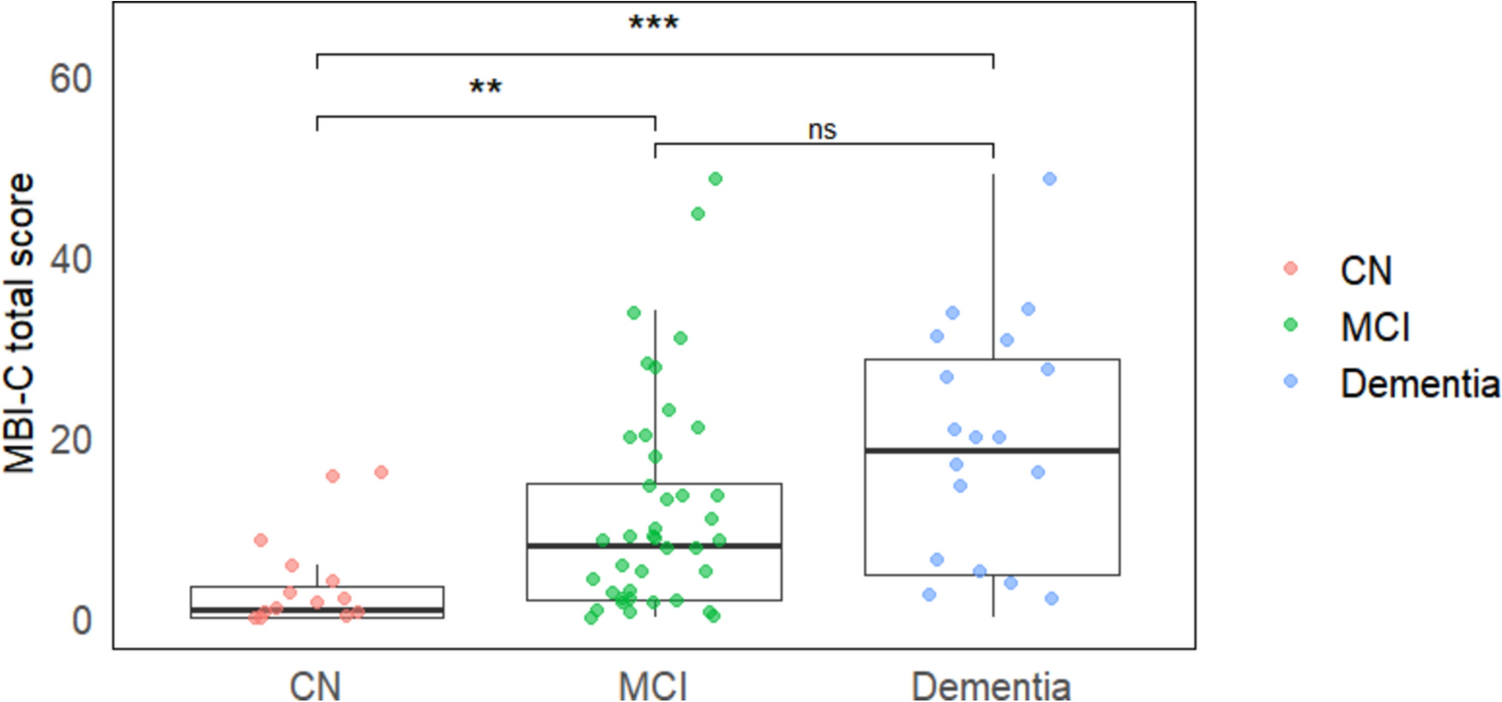
Table 1 Characteristic of the subject with Lewy body disease (LBD) continuumMBI across the LBD continuumThe MBI-C total score showed significant differences among the three groups, with an increasing trend from CN to MCI, and then to dementia groups (p < 0.001) (Table 2, Fig. 1). In the MBI-C subdomains, significant group differences were observed, with the most pronounced differences noted in the subdomains of decreased motivation, affective dysregulation, and impulse dyscontrol.
Table 2 Comparison of MBI-C total and subdomain scores across the LBD continuumFig. 1
MBI-C total scores of LBD continuum. The MBI-C total score showed a statistically significant increasing trend across the three groups, with significant differences between CN and MCI groups, and between CN and dementia groups (p < 0.001). ** p < 0.01, *** p < 0.001, ns; not significant
We performed partial correlation analyses in the entire LBD continuum subjects, controlling for age and sex to assess the relationship between the MBI-C total score and various clinical indices (Table 3). Significant associations were found with GDS, K-MMSE, and the MDS-UPDRS parts 1, 2, 3, and total scores. Regarding neuropsychological tests, significant correlations were observed in domains such as attention (TMT-A; r = −0.343, p = 0.002), language (K-BNT; r = −0.354, p = 0.001), memory (SVLT immediate recall; r = −0.250, p = 0.026), and frontal/executive functions (DSC; r = −0.314, p = 0.006, TMT-B; r = −0.339, p = 0.003). When partial correlation analysis was applied to subgroups within the LBD continuum, slight variations in the patterns of associations across groups were noted. In the LBD-CN group, significant correlations were observed with GDS (r = 0.505, p = 0.039), and the frontal/executive function domains, specifically COWAT phonemic (r = −0.482, p = 0.036) and COWAT semantic (r = −0.477, p = 0.039). The LBD-MCI group showed significant associations with the MDS-UPDRS parts 1, 2, 3, and total scores, as well as with attention (TMT-A; r = −0.311, p = 0.040) and frontal/executive functions (DSC; r = −0.329, p = 0.033, TMT-B; r = −0.303, p = 0.048). In the Lewy body dementia group, correlations were found with the MDS-UPDRS total score (r = 0.568, p = 0.022), global cognition as measured by the K-MMSE (r = −0.582, p = 0.018), and verbal memory function (SVLT delayed recall; r = −0.719, p = 0.003).
Table 3 Association of MBI-C total score with clinical indices across the entire LBD continuum and its subpopulationsFor differentiating MCI from CN in the LBD continuum, the area under the curve (AUC) of the MBI-C was found to be 0.736 [95% confidence interval (CI) = 0.607–0.965, p = 0.001], with an optimal cutoff point of 5.0, sensitivity of 60.0%, and specificity of 78.9%.
MBI as a risk marker in iRBDThe iRBD group was categorized into two subgroups based on the presence or absence of multiple prodromal markers. Out of the 35 total iRBD patients, 11 were classified into the iRBD-low risk group, while 24 were categorized into the iRBD-enriched risk group. Detailed demographics and clinical features are presented in Supplementary Table 1. All six prodromal markers were more prevalent in the iRBD-enriched risk compared to low risk groups, with significant differences in MPS (p = 0.003), constipation (p = 0.002), and orthostatic dizziness (p = 0.038) (data not shown). The MBI-C total score was higher in the iRBD-enriched risk group. The MBI-C’s five subdomains showed notable distinctions, particularly in the domain of impulse dyscontrol (p = 0.003). The MDS-UPDRS parts 1, 2, 3, and total scores were all significantly higher in the iRBD-enriched risk group, a pattern that was also observed in the K-SCOPA-AUT total score. In neuropsychological tests, the iRBD-enriched risk group exhibited a non-significant tendency of lower performance in the frontal/executive function than the iRBD-low risk group (supplementary Table 1). There was no significant relationship between the RBD symptom duration and MBI in iRBD patients (data not shown).
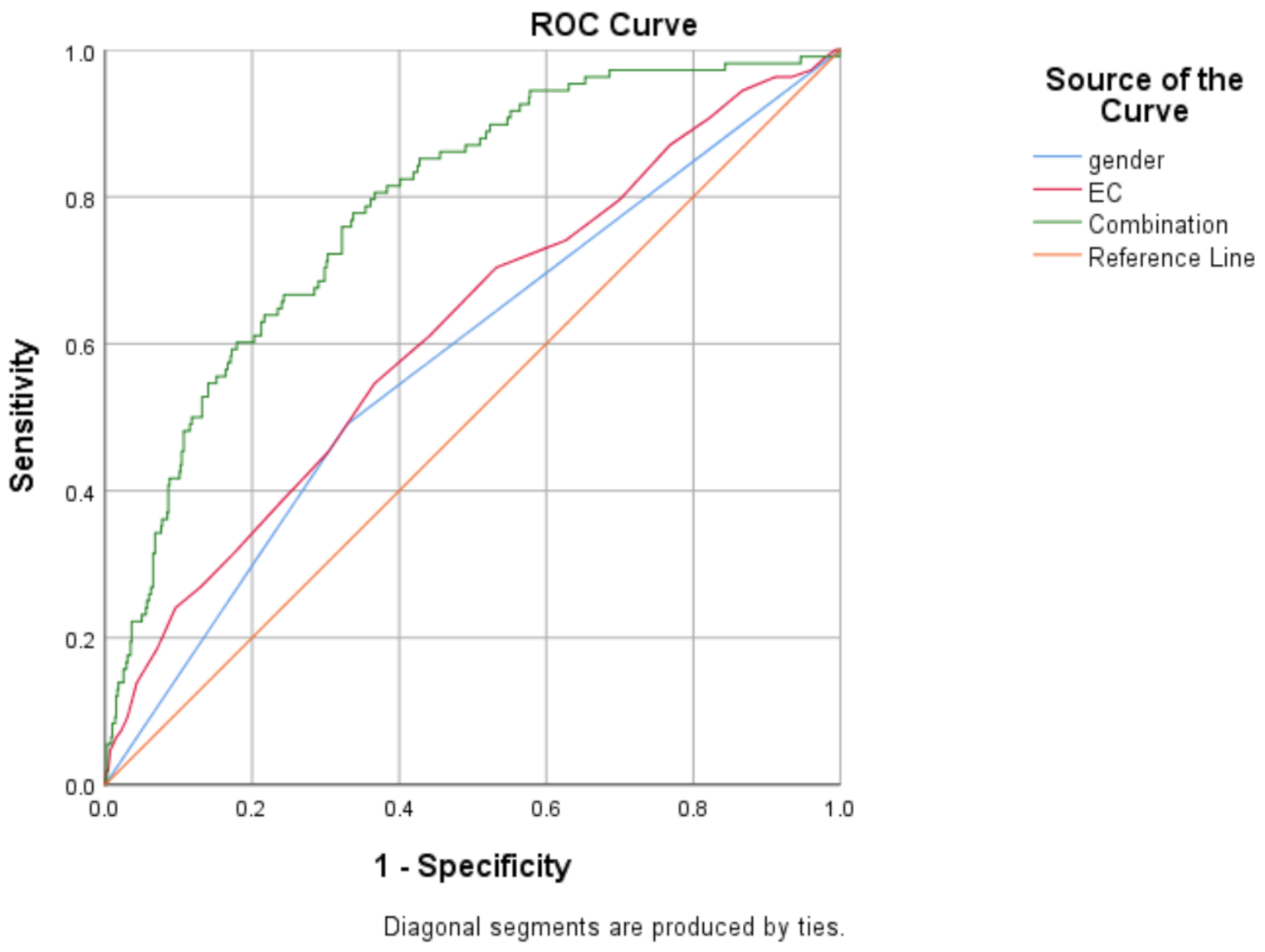
For discriminating the iRBD-enriched risk against the low-risk groups, ROC analysis revealed that the AUC of the MBI-C was 0.720 [95% CI 0.559–0.881, p = 0.018]. The optimal cut-off point of the MBI-C was 4.0, with a sensitivity of 58.3% and a specificity of 90.9%.
留言 (0)