Study design
This controlled, randomized, double-blind, cross-over clinical trial was conducted at the University Medical Center Hamburg-Eppendorf and compares the effect of STN-DBS and combined STN + SNr-DBS as described previously (Hidding et al. 2017; Pflug et al. 2020). The study was approved by the local ethics committee and was conducted in agreement with the Code of Ethics of the World Medical Association (Declaration of Helsinki, 1967). Written informed consent was obtained from all participants. Patients were examined by a non-blinded therapeutic movement disorder specialist, who programmed the stimulation conditions, and by a blinded phoniatric examiner at three visits each three weeks apart. All visits were performed in medication-on condition.
Stereotactic procedures
Detailed description of DBS surgery for optimal target site localization for electrode implantation by MR-based stereotactic planning, microrecording and stimulation has been described previously (Steigerwald et al. 2008). Electrode position at the upper border of the SNr was defined as location of the electrode tip at least 4.5–6 mm inferior to AC-PC line. The position of the implanted electrodes (model 3389; Medtronic, Minneapolis, Minnesota, USA, in 8 cases, and 8-poled electrode model, Boston Scientific, Valencia, CA, USA, in 2 cases) was determined by coregistration of the preoperative T1-MRI-scans and post-operative CT-scans performed with Brainlab (iPlan software; Brainlab, Feldkirchen, Germany).
DBS settings
After testing thresholds for side effects in the SNr, defined stimulation settings for the STN and STN + SNr stimulation were fixed for the course of the experiment. The STN settings did not differ from those before the study in everyday life condition. Afterwards, stimulation of the STN or combined STN + SNr was set in a randomized manner for the following 3 weeks. Speech and voice examinations were performed in the following order:
Firstly, patients were investigated at baseline visit with DBS switched off (STIM-OFF) mode.
(I)
In phase I, patients were examined after random assignment to one of two DBS modes: conventional STN-DBS or combined STN + SNr-DBS.
(II)
After 3 weeks, reprogramming was performed in a cross-over procedure for the following 3 weeks. In this phase II, the third evaluation of the patients occurred as described before (Pflug et al. 2020).
Patients were blinded for their stimulation condition (conventional STN stimulation or combined STN + SNr stimulation). At the end, patients were unblinded and the preferred stimulation condition was programmed as permanent therapeutic stimulation. Medication and stimulation parameters were held constant during the phase I and II of the study. Only in one case, the stimulation amplitude in the SNr had to be reduced after 2 days due to dyskinesias.
Subjects
15 patients suffering from PD participated in the study. Four patients withdrew from the study due to side effects of combined STN + SNr-DBS. Side effects of nigral costimulation were worsening of motor functions as well as a lack of beneficial effects of levodopa, akathisia, general uncomfortable feeling, aggressiveness, and increased confusion and hallucinations during chronic stimulation. The results of the 11 patients, who completed the full study protocol, were considered. Demographic and clinical characteristics are described in detail in Table S1 and in a previous publication (Pflug et al. 2020). The gender distribution of male:female was 10:1 and the mean age was 63.5 years (range 53–74). Mean disease duration was 12.0 ± 5.0 years and mean Hoehn & Yahr stage 2.2 ± 0.36.
All patients had a bilateral STN-DBS with the deepest contacts of the electrodes within the dorsal aspects of the SNr along image-based electrode reconstruction (> 4.5 mm below AC-PC). The study inclusion and exclusion criteria, as well as the selection criteria for DBS surgery, have been reported in detail previously (Hidding et al. 2017). The location of the electrode contacts was controlled by stereotactic coordinates based on MR imaging and intraoperative microrecording. The mean stereotactic coordinates of the ventral most DBS contact relative to the mid-commissural point of the 11 PD patients (mean ± standard deviation in mm) were x = 10.4 ± 0.9, y = 2.8 ± 1.3, z = 6.3 ± 1.0 for the left hemisphere and x = 10.1 ± 1.7, y = 2.7 ± 1.5, z = 5.7 ± 1.4 for the right side (x = lateral to midline, y = posterior to MCP, z = inferior to AC-PC level, see Fig. S1 in the Supplement).
Assessments and speech and voice analysis
To evaluate the effects of a combined STN + SNr stimulation on speech and voice function and the patients´ self-perception, clinical examination and speech and voice analysis were performed.
Since there are no standards or guidelines for voice diagnostics in PD, this study partially followed the protocol of Rusz et al. (Rusz et al. 2020). Speech and voice were analyzed subjectively using questionnaires and objectively using audio analysis.
Subjective evaluation of speech and voice
All patients completed the validated questionnaires Speech Handicap Index (SHI) (Rinkel et al. 2008) and Voice Handicap Index (VHI) (Rosen et al. 2004), each in the German language version. The SHI and VHI are standardized questionnaires validated in many languages to measure the impact of speech and voice problems on a patient's quality of life (low values indicate a lower handicap; items relate to shame, effort, stress, avoidance, anger).
In addition, perceived voice quality (a) and pronunciation quality (b) on that day were assessed on a 10 cm visual analog scale (VAS) by the patients. A score below 30% on the VAS was classified as acceptable voice and pronunciation quality in the respective case.
Objective evaluation of speech and voice
Vocal tasks The speech and voice analysis consisted of three vocal tasks, namely a reading passage, a sustained vowel, and sequential and alternating motion rates.
Sustained vowel: the patient produces vowel [a] at comfortable pitch and loudness as long as possible, max. two repetitions to improve the result.
Reading passage: the patient reads the short standard text "The North Wind and the Sun" by Aesop (in German—"Nordwind und Sonne”) in a comfortable pitch and loudness.
Sequential and alternating motion rates (diadochokinesis): the patient produces syllables [pa] and [pataka] as fast as possible on one breath with max. two repetitions to improve each result.
In all patients, the three diagnostic tasks were performed in all three conditions, STIM-OFF, Phase I, and Phase II with respective STN-DBS or STN + SNr-DBS, respectively.
Audio recording and processing
The tasks were recorded using the SpeechStudio system (Laryngograph Ltd., London). This was done in a pseudo-random order to avoid bias due to decreasing patient endurance. The signal-to-noise ratio of background noise in the room and voice loudness was checked to be > 30 dB, as recommended by Deliyski et al. (2005). The sample rate was 16 kHz, the amplitude resolution was 16 bits. The system records the microphone signal at 30 cm distance to the mouth of the examined person in uncompressed WAV format. The optimal recording level was set manually during a test recording.
The Praat system, version 6.1.38 (Boersma and Weenink 2021), was used for all audio processing.
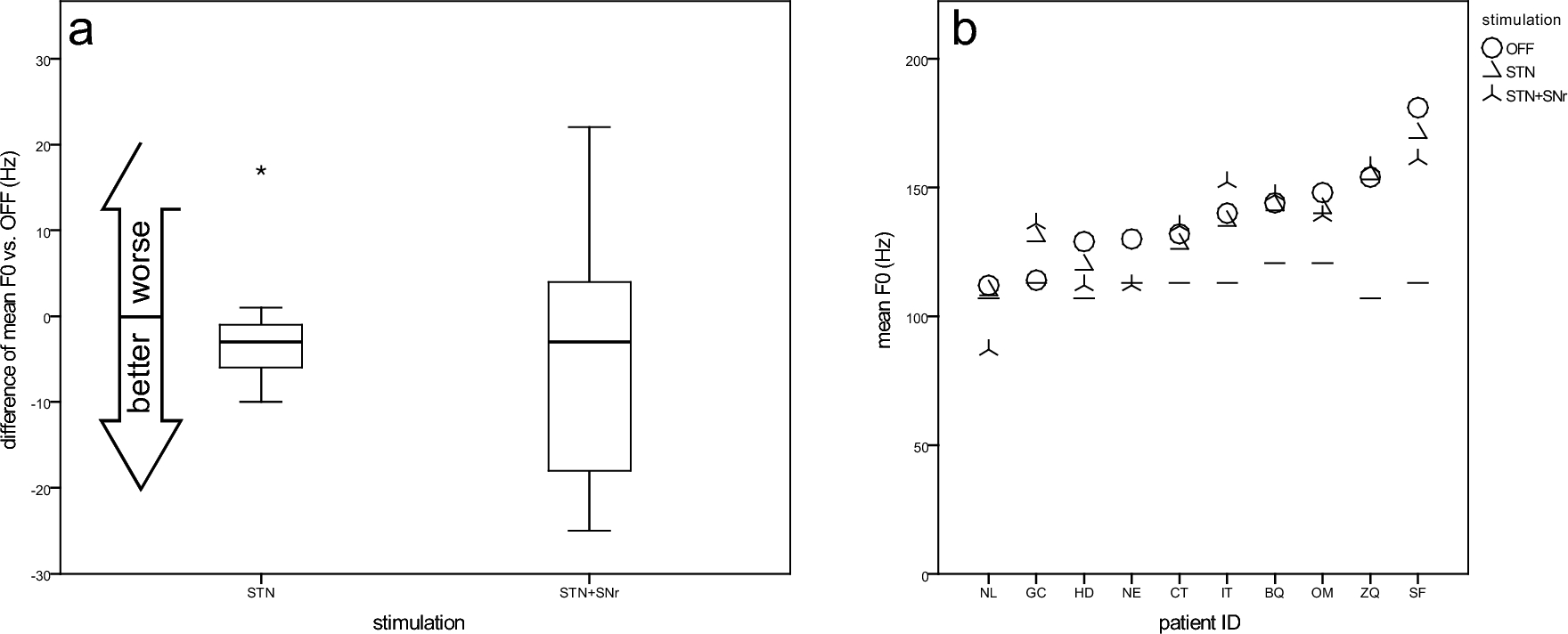
The mean fundamental frequency (F0), the main contributor to auditory perception of vocal pitch, was extracted from the standard text recording by the Praat function “To pitch…” (automatic time step, pitch floor/ceiling at 75/300 Hz) and the Praat function “Get mean…” and measured in Hertz (Hz). As a measure of speech intonation, the F0 variation coefficient was calculated from the quotient of F0 standard deviation (Praat function “Get standard deviation…”) and mean fundamental frequency.
The maximum syllable rate for [pa] and [pataka] was measured using a digital Praat program script (Mayer 2021) and adjusted based on the Praat sound intensity function “Get value in frame…”. The script suggested the most likely syllable boundaries which had to be confirmed by visual inspection of the boundaries in a spectrogram plot. The script determined the rate value for each task by extracting the mean rate of the fastest 5 subsequent syllables.
The reading time (RT) was measured manually from the task “reading passage” analogous to the MPT in the plot of the time signal.
The maximum phonation time (MPT) for the “sustained vowel” was measured as the duration of vowel [a] produced on one breath. The MPT will be reduced in persons with reduced lung capacity or disturbed voice. A critical threshold was set to 12 s from clinical experience, but without evidence from literature, as the parameter suffers from many side effects (Baken and Orlikoff 2000).
For the acoustic measure of voice quality, the Acoustic Voice Quality Index (AVQI) value (Maryn et al. 2010) was determined by the corresponding Praat script with version 03.01 and following the procedure described by Barsties et al. (2018). It uses 3 s of the sustained vowel sound and the first 27 syllables of the reading passage (Barsties von Latoszek et al. 2020), which in this study had a mean length of 6.8 s. The AVQI combines several acoustic parameters to one index, which shows bigger values for disturbed (hoarse) voices. The threshold for distinction between normophonic and dysphonic was set to 1.85, according to Barsties et al. (2020) for German language.
Correlation with TEED
All speech and voice parameters were correlated with the total electrical energy delivered by DBS (TEED). This parameter is calculated from the DBS stimulation parameters. It is the product of the (1) squared impulse amplitude, (2) the impulse width, and (3) the impulse frequency as described by Moreau (Moreau et al. 2008).
Statistics
Group differences were tested with the t-test for connected samples. The significance level was set to 0.05.

留言 (0)