
記住我
With a sample size of 115 SD patients, our study is one of the largest studies of its kind. It is, so far, the only study focusing on SD and its relationship with other neurological symptoms of dystonia.
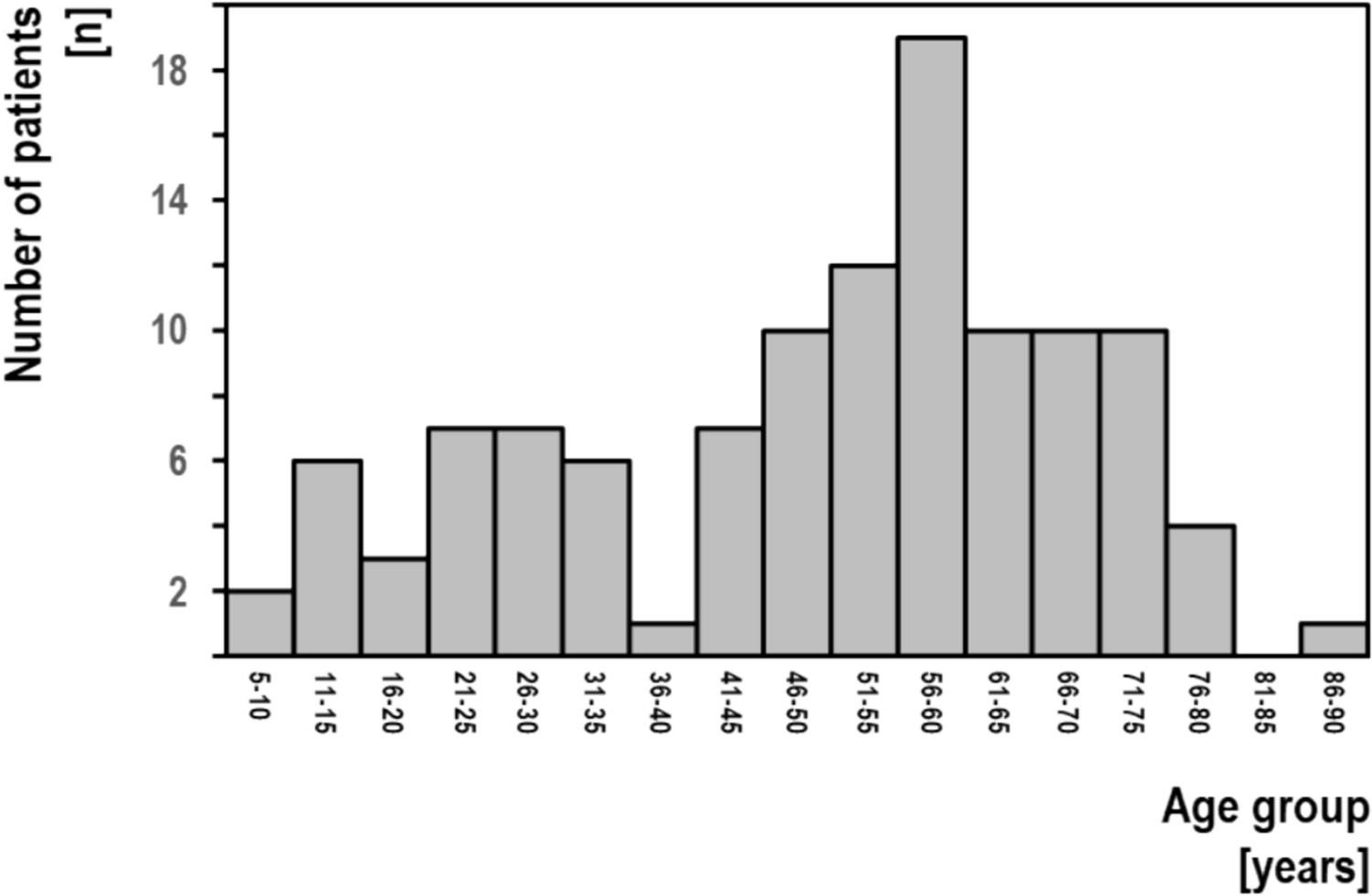
Patient demographicsOur study shows a patient age at SD onset of 49.9 ± 19.1 years with a range of 6–68 years. This is similar to previously reported data ranging from 44 to 50 years (Tanner et al. 2011; Aronson et al. 1968; Schweinfurth et al. 2002; Brodnitz 1976). Obviously, the patient age at SD onset is different from the patient age at study inclusion and both data shouldn’t be confused. In our group, the patient age at study inclusion was 69.3 ± 16.3 years. As shown in Fig. 1, there are a number of patients with early onset. Some of these patients presented with perinatal brain damage, others might represent cases with strong genetic aetiology known to manifest early.
Fig. 1
Onset of spasmodic dysphonia
In our study, SD prevalence was reported as 24.7 per million population, making it the eighth most common form of dystonia with 3% of all dystonia manifestations. Claims of SD being the third most common form of focal dystonia are over-estimates and obviously blurred by methodological flaws (Castelon-Konkiewitz et al. 2002).
Our study also shows a strong female predominance of 2.0. Previously reported female/male ratios range from 1 to 7 (Nutt et al. 1988; Schweinfurth et al. 2002, Blitzer et al. 2018, Adler et al. 1997). Our figure is in line with a similar female predominance recently reported in other idiopathic focal dystonias (except for musician’s dystonia) (Dressler et al. 2022).
A family history of dystonia was identified in 17% of our SD patients including SD and a large variety of other focal, segmental or generalised dystonia manifestations. For SD, 3% of of our SD patients had a family history. Previous data on the family history of dystonia are sparse, suggesting a frequency of 12% for all forms of dystonia (Blitzer et al. 2017), a 'very low' frequency for SD (Ludlow 2010) or a non-existent one for SD (Schweinfurth et al. 2002). Reasons for these discrepancies, especially for non-SD dystonias, are likely to be patient evaluations performed by experts lacking up-to date expertise in movement disorders, especially dystonia.
Clinical symptomatologyDescriptions of the relative frequency of SD subforms in the literature are surprisingly vague. Unanimously, SD-AD is believed to be by far the most common form of SD with a frequency of around 80% to 90% (Ludlow 2010, Edgar et al. 2001; Hyodo et al. 2021, Blitzer et al. 2017), whereas SD-AB is thought to be rare (Ludlow 2010) with frequencies of around 15% (Edgar et al. 2001, Blitzer et al. 2017). Figures for SD-M are not readily available. Our study revealed contrasting relative frequencies of SD-AB of 31%, of SD-AD of 28% and of SD-M of 41%. Reasons for this discrepancy are not immediately clear. First of all, our combined neurological and phoniatric approach retrieved an entirely different patient population with much higher frequencies of additional dystonia manifestations and family histories of dystonia than previously reported. Mainly, however, this observation seems to reflect previous terminological confusion, especially with respect to essential tremor, which is a separate clinical entity characterised by isolated tremor not associated with any dystonic elements, occurring on action, but not being task-specific and predominantly affecting the upper extremities. If voice tremor is misdiagnosed as essential tremor, as it was in the past, these patients were excluded from the spectrum of SD. In our study population, 30% of all SD-M patients had dystonic voice tremor, whilst essential voice tremor could not be detected. 6% of our SD-AB patients presented with voice tremor. Whether dystonic voice tremor without any tonic spasmodic dysphonation may exist, is unclear. Considering our combined observations, we suggest that SD is classified according to its tonic dystonia elements as SD-AD, SD-AB and SD-M. Dystonic tremor may be superimposed. Pure dystonic tremor of the larynx may exist.
Whereas in our study 63% of all SD patients had additional dystonia manifestations, this frequency was previously reported with around 16% (Blitzer et al. 1998). Around 30% of SD patients are reported to have additional vocal tremor (Ludlow 2010, Tanner et al. 2011; White et al. 2011; Schweinfurth et al. 2002). This tremor was believed to represent the co-existence of SD and essential tremor. In our study, the frequency of tremulous SD was 14%, similar to previously reported figures. However, it was not caused by essential tremor. Instead, it reflected dystonic tremor, as all patients with tremulous SD had dystonia manifestations elsewhere in the body and all patients with tremulous SD had tonic dystonic laryngeal muscle involvement and some had gestes antagonistes or other sensory tricks.
Confusion about the nature of tremor syndromes is common and reflects classificatory deficits from times, before the dystonia concept was developed and the role of dystonic tremor became apparent. Although we are not challenging the existence of ET affecting laryngeal muscles, we believe that this is rare. The same might be true for Parkinsonian tremor. For SD patients initially diagnosed in our department, there could be a possible bias favoring the prevalence of dystonia, as our main expertise is perceived by referral partners to be dystonia and botulinum toxin therapy. However, half of the SD in our study were initially seen in the Department of Phoniatry, where this bias did not exist.
留言 (0)