
記住我
Two-hundred-and-forty R/R AML patients were treated with HMA and off-label VEN between January 2017 and April 2023 and were included in our analysis (entire cohort). Table 1 provides details on clinical characteristics at the time of treatment with HMA/VEN. The median age was 68.6 years (range, 20-88). A similar proportion of patients had relapsed (n = 110; 46%) or had refractory disease (n = 130; 54%). ELN 2022 risk was favorable, intermediate and adverse in 5%, 20%, and 57% of patients, respectively. Patients had a median of two prior treatment lines (range, 1–7), including 67% patients with intensive pretreatment and 36% with prior alloHCT. The majority of patients received azacitidine (80%) combined with VEN, while 20% received decitabine (Table 2). Median VEN dose after ramp-up was 100 mg (range, 50–600 mg) and 121 patients (50%) received VEN for 14 days.
Table 1 Demographic and disease characteristics of patients with relapsed/refractory AML treated with HMA/VEN.Table 2 Treatment characteristics of patients with relapsed/refractory AML treated with HMA/VEN (entire cohort).For 174 patients (73%) molecular data were available (molecular cohort, Supplementary Fig. S1).
Most commonly mutated genes included those associated with clonal hematopoiesis (TET2 20%, ASXL1 18%, DNMT3A 17%) besides RUNX1 (19%), and TP53 (18%), whereas 19 patients (11%) had no detectable mutation. Among those, three patients had a complex karyotype, three had KMT2A-rearranged AML and two had single cytogenetic aberrations, while the remaining 11 (6%) patients had no detectable cytogenetic aberration. Median variant allele frequencies (VAF) are depicted in Supplementary Fig. S2, indicating lower VAFs in genes that are involved in signaling pathways such as FLT3-ITD, NRAS and PTPN11, whereas higher VAFs were observed in splicing genes (SRSF2, ZRSR2) and transcription factors (RUNX1).
Treatment response and outcome in the entire cohortPatients received a median of 2 treatment cycles (range 1-34) of HMA/VEN. CR and CRi rates were 25% and 14%, respectively. The overall response rate (ORR) was 44%, including 39% of patients with CR/CRi and 5% of patients with MLFS (Table 3). Partial remission was achieved in one patient, while 45% of patients (n = 108) did not respond to HMA/VEN. Twenty-five patients (10%) died before response assessment was performed (Table 3). CR/CRi rates were higher in patients with white blood cell (WBC) count ≤5 × 109/L (46% vs 25%; p = 0.002) and platelet count >30 × 109/L (46% vs 30%; p = 0.01), while all other characteristics did not associate with response (Supplementary Table S1).
Table 3 Treatment response of patients with relapsed/refractory AML treated with HMA/VEN (full cohort N = 240 and molecular cohort n = 174).After a median follow-up of 31.5 months, median OS was 7.9 months (95% CI, 6.4–10.2 months) and median EFS was 5.1 months (95% CI, 4.4–6.3 months) in the entire cohort. In CR/CRi patients median RFS was 12.9 months (95% CI, 10.2 months to not reached) (Fig. 1A–C).
Fig. 1: Kaplan–Meier estimates for survival for the entire cohort (N = 240).
A Kaplan–Meier estimates for overall survival. B Kaplan–Meier estimates for event-free survival. C Kaplan–Meier estimates for relapse-free survival in CR/CRi patients.
Clinical and molecular signatures of responseOne-hundred-seventy-four patients with molecular data were evaluated for clinical and molecular predictors of response. In univariate analysis, CR/CRi was more likely to occur in patients with WBC count ≤5 × 109/L (46% vs 20%; p = 0.02) and platelet count >30 × 109/L (41% vs 29%; p = 0.05) (Supplementary Table S2).
Molecular predictors of inferior response included mutated PTPN11 (mutated vs wildtype (wt) CR/CRi 0% vs 38%; p = 0.06). Mutated NF1 and TP53 were numerically associated with inferior response (NF1 mutated vs wt CR/CRi 14% vs 37%; p = 0.2; TP53 mutated vs wt CR/CRi 29% vs 38%; p = 0.36), whereas mutated IDH2 (mutated vs wt CR/CRi 46% vs 34%; p = 0.2) or STAG2 (mutated vs wt CR/CRi 53% vs 34%; p = 0.13) status were numerically associated with a higher rate of CR/CRi (Supplementary Table S3).
Predictors of overall and event-free survivalWe next evaluated clinical and molecular markers for associations with OS and EFS. In univariate analysis of pretreatment variables, predictors of inferior OS included age >70 years (HR 1.38 95% CI 1.0-1.98; p = 0.064), the presence of extramedullary disease (HR 2.06, 95% CI 1.33–3.2; p = 0.001), HMA pretreatment (HR 1.63, 95% CI 1.15–2.3; p = 0.006), higher WBC count (HR 1.38 95% CI 0.92–1.94; p = 0.12) and complex karyotype (HR 1.33, 95% CI 0.91-1.94; p = 0.14) (Supplementary Fig. S3, Supplementary Table S4). Predictors for inferior EFS further included the type of combination partner (decitabine vs. azacitidine: HR 1.48, 95% CI 1.02–2.13; p = 0.038). Molecular predictors of inferior OS included mutations in NF1 (HR 2.53, 95% CI 1.2–5.4; p = 0.015), PTPN11 (HR 2.26, 95% CI 1.5–3.4; p < 0.001), TP53 (HR 1.5, 95% CI 0.96–2.3; p = 0.073), and FLT3 (any FLT3 mutation, HR 1.64, 95% CI 1.00–2.7; p = 0.05) (Supplementary Fig. S4, Supplementary Table S5). The number of prior treatment lines was not a significant parameter in univariate analysis for OS and EFS (Supplementary Table S5; Supplementary Fig. S5) and was not further considered. In multivariate analysis extramedullary disease (HR 2.46, 95% CI 1.5–4.0; p = <0.001), HMA pretreatment (HR 1.9, 95% CI 1.3-2.8; p < 0.001), presence of PTPN11 (HR 2.2, 95% CI 1.3–4.0; p = 0.006), and NF1 (HR 2.26, 95% CI 1.5–3.4; p < 0.001) mutations were identified as independent risk factors for inferior OS, whereas presence of SF3B1 mutations (HR 0.38, 95% CI 0.2–0.8; p = 0.01) remained as independent risk factor for superior OS (Table 4). Independent risk factors for inferior EFS were similar to those for OS and included extramedullary disease (HR 1.76, 95% CI 1.1–2.8; p = 0.02), HMA pretreatment (HR 1.57, 95% CI 1.1–2.2; p = 0.014), and presence of mutations in PTPN11 (HR 2.1, 95% CI 1.1–4.03; p = 0.03), and FLT3 (HR 1.82, 95% CI 1.1–3.04; p = 0.02). Presence of a SF3B1 mutation was associated with superior EFS (HR 0.42, 95% CI 0.2–0.8; p = 0.01) (Table 4).
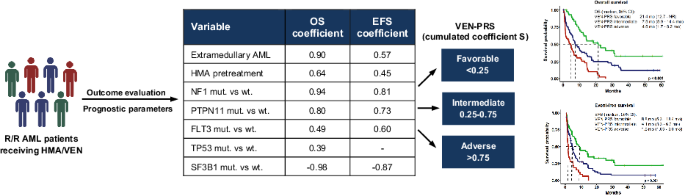
Table 4 Uni- and multivariate analyses for overall survival (OS) and event-free survival (EFS) of molecular markers for OS and EFS in 174 acute myeloid leukemia (AML) patients.Subsequently, a three-tiered risk stratification model was developed for OS and EFS based on HR-weighted scoring. For OS the following variables were included in the model: extramedullary AML, HMA pretreatment, mutated PTPN11, FLT3, TP53, NF1, and SF3B1. Each variable was weighted by calculating the hazard coefficient, which is the natural logarithm of the hazard ratio of the variable (Table 4). The individual score for each patient was calculated by adding up the coefficients of variables that apply for each individual patient. Based on the individual score, patients were stratified into three risk groups: patients with a VEN-PRS of <0.25 were assigned to the favorable risk group, patients with a VEN-PRS between 0.25 and 0.75 to the intermediate risk group, and patients with VEN-PRS > 0.75 to the adverse risk group (Supplementary Fig. S6A). When applying the newly developed VEN-PRS, it allocated 46 (26%), 75 (43%), and 53 patients (31%) into the favorable-, intermediate-, and adverse risk groups, respectively with significant differences in OS (median OS, 95% CI in favorable vs intermediate vs adverse risk groups: 14.2 months (10.2–31.1) vs 7.0 months (5.0–13.2) vs 3.1 months (1.5–6.7); p < 0.001) (Fig. 2).
Fig. 2: Kaplan–Meier estimates for overall survival of 174 patients with molecular information according to VEN-PRS classification.
Favorable risk: SOS < 0.25; intermediate risk: 0.25 ≤ SOS ≤ 0.75; adverse risk: SOS > 0.75.
For EFS the following variables were included to the model: extramedullary AML, HMA pretreatment, mutated PTPN11, FLT3, NF1, and SF3B1. Based on the individual scores patients were stratified into three risk groups for EFS analogous to OS (Supplementary Fig. S6B). The VEN-PRS model allowed to allocate patients into three risk groups with significantly different EFS (median EFS, 95% CI in favorable vs intermediate vs adverse risk group: 8.8 months (6.3–18.43) vs 4.1 months (3.33–6.2) vs 1.8 months (1.03–3.03); p < 0.001) (Fig. 3). One-, two-, and three-year OS and EFS are provided in Supplementary Table S6. Supplementary Table S7 provides the VEN-PRS calculator for estimating patient’s individual risk.
Fig. 3: Kaplan–Meier estimates for event-free survival of 174 patients with molecular information according to VEN-PRS classification.
Favorable risk: SEFS < 0.25; intermediate risk: 0.25 ≤ SEFS ≤ 0.75; adverse risk: SEFS > 0.75.
The VEN-PRS was evaluated separately in the relapsed and refractory cohorts and was similarly prognostic in these subgroups (Supplementary Figs. S7 and S8). The VEN-PRS was also prognostic in patients treated with HMA/VEN after one prior line of treatment for OS, but not EFS (Supplementary Fig. S9), and it was prognostic in patients treated with HMA/VEN after more than one prior line of treatment for both OS and EFS (Supplementary Fig. S10).
Calibration analysis showed that the predicted 10-month survival correlated well with the observed survival for the three risk groups, where EFS in the adverse risk group is somewhat underestimated, confirming that the model is well calibrated (Supplementary Fig. S11). In discrimination analysis, the AUC was 0.67 for OS and 0.68 for EFS, corresponding to a moderate discrimination (Supplementary Fig. S12).
As we did not have access to a second R/R AML cohort treated with venetoclax for external validation, we evaluated our score in patients treated with HMA/VEN at first diagnosis (n = 189). There were less patients in the adverse risk group since a significantly lower number of patients in the first-line cohort had prior HMA treatment (first-line n = 22; R/R AML n = 99) and extramedullary manifestation (first-line n = 4; R/R AML n = 17) (Supplementary Table S8), but the model showed significantly different risks for the favorable, intermediate and adverse risk groups for OS and for the favorable and intermediate risk groups for EFS, thus independently validating the VEN-PRS (Supplementary Figs. S13A and S13B). AIC differences are negative with -6.14 for OS and -6.94 for EFS, showing that our variable selection is suitable for modeling an independent cohort.
Taken together, our analyses suggest HMA pretreatment, extramedullary disease and the mutation status of NF1, PTPN11, FLT3, TP53 and SF3B1 as clinically relevant predictors of survival in patients treated with HMA/VEN for R/R AML.
Comparison of VEN-PRS to other AML risk modelsWe first compared our prognostic score model with the prognostic index proposed by Breems and colleagues [12], which was developed to estimate the outcome of AML patients in first relapse. The prognostic index showed no significant fit to our data. The AIC difference between the prognostic index by Breems et al. and the null model was 3.72 and 3.97 for OS and EFS, respectively, whereas the AIC difference between our proposed model and the null model was −26.67 and −20.11 for OS and EFS, respectively. As a more negative AIC difference indicates less prognostic information loss, our model clearly outperforms the prognostic index by Breems (Supplementary Fig. S14).
We next evaluated the ELN2022 risk classification, which was developed for newly diagnosed AML patients undergoing intensive chemotherapy and thus is not expected to be prognostic in R/R patients [3]. CR/CRi rates were 42%, 44%, and 33% in favorable, intermediate, and adverse ELN2022 risk patients, respectively (p = 0.44). Overall survival in the context of ELN2022 in the favorable, intermediate, and adverse risk groups was 11.1 months, 8.4 months, and 9.3 months, respectively (p = 0.9). The AIC difference between the ELN2022 classification and the null model was 3.8 and 3.91 for OS and EFS, respectively.
We then evaluated the VIALE A prognostic score proposed by Döhner and colleagues [25], which stratified newly diagnosed HMA/VEN treated patients into three risk groups based on the mutational status of four genes (favorable: TP53 wt, no FLT3-ITD, K/NRAS wt; intermediate FLT3-ITD or K/NRAS mutated; adverse TP53 mutated) [24]. Median OS rates in favorable, intermediate, and adverse risk groups were 7.6 months, 12 months, and 8.2 months (p = 0.18), respectively, when applying the VIALE A prognostic score on our cohort of R/R AML patients (Supplementary Fig. S15). The AIC difference between the proposed VIALE A prognostic score and the null model was 0.90 and 0.32 for OS and EFS, respectively.
Lastly, we further compared our prognostic model with the recently published score by Gangat and colleagues, which stratified newly diagnosed patients undergoing HMA/VEN treatment into three risk groups based on HR-weighted scoring of the following parameters: failure to achieve CR/CRi, adverse karyotype, TP53 mutation, and absence of IDH2 mutation. Reported mOS were 28.9, 9.6, and 3.1 months for the low, intermediate and high-risk groups, respectively for AML patients treated with frontline HMA/VEN [26]. Applying the score on our R/R AML cohort, survival estimates in favorable, intermediate, and adverse risk groups were 24.1 months, 6.7 months, and 4.6 months (p < 0.001), respectively (Supplementary Fig. S16). While this model provided good separation in the R/R setting, the AIC difference between the proposed score by Gangat et al. classification and the null model was −16.03 for OS and thus performed less well compared to the proposed VEN-PRS model.
In summary, previously published risk scores and classifications showed significantly lower accuracy in predicting outcomes of R/R AML patients treated with HMA/VEN compared to our proposed risk model, suggesting that other risk factors than the previously established pre-treatment characteristics determine efficacy of HMA/VEN in R/R AML patients.
留言 (0)