
記住我
The median age at diagnosis of POEMS syndrome of the 49 decedents was 56 years (IQR 43, 60), and median age at death was 64 years (IQR 54, 70) (Supplementary Table 1). Patients were diagnosed between 1981 and 2020. By definition, all patients had evidence of both peripheral polyneuropathy and monoclonal plasma cell proliferative disorder. All but 1 patient had a lambda restricted clone. Eighty-six percent of patients had endocrinopathy, sclerotic or mixed sclerotic and lytic bone lesions (84%), and extravascular volume overload (69%). Thrombocytosis and extravascular volume overload were more common in those with known cause of death.
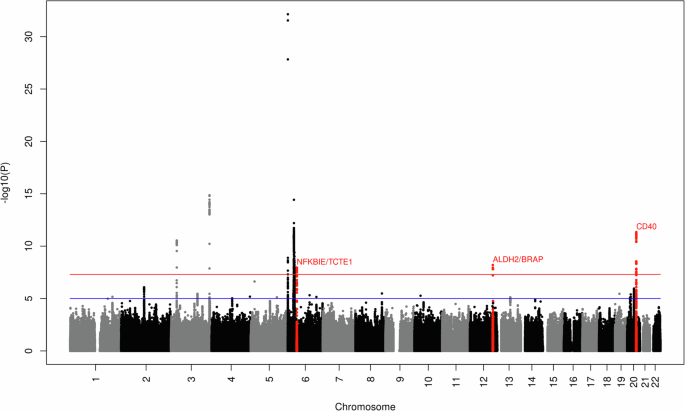
Cause of death in POEMS syndromeThe distribution of cause of death is shown in Fig. 1. Thirty-two (65%) patients died related to POEMS syndrome or its therapy, and 17 (35%) died from unrelated causes or from second primary malignancy (Table 1). By definition, the unrelated causes of death occurred among patients in the observation phase for their POEMS syndrome. These unrelated causes included 6 fatal second primary malignancies comprising 2 instances of metastatic lung cancer and one each of hepatocellular carcinoma, prostate carcinoma, leiomyosarcoma, and metastatic GI neuroendocrine tumor. The remaining 11 unrelated causes of death included pneumonia in 3, heart failure in 3, and one instance each of dementia, sudden death, stroke, intracranial hemorrhage after a fall, and suicide. These 17 patients whose death was not attributed to POEMS or its treatment were diagnosed in a slightly earlier period (median diagnosis year 2003 versus 2004, p = 0.04) and at presentation were more likely to have erythrocytosis (50% versus 21%, p = 0.07), had fewer bone marrow plasma cells (4% versus 5%, p = 0.02), and were more likely to have received radiation as part of their therapy (59% versus 34%, p = 0.05) (Table 1). Median time to death for those dying of unrelated causes versus due to complications of POEMS syndrome or its treatment was 12.5 years (95% CI 6.7, 18.4) versus 3.9 years (95%CI 1.3, 9.3), p = 0.002 (log-rank), (Fig. 2a).
Fig. 1
Causes of death in patients with POEMS syndrome.
Table 1 Baseline characteristics by whether death was POEMS or treatment related.Fig. 2: Time to death by cause of death (COD).
Time to death from diagnosis in (A) patients who died related to POEMS syndrome (n = 32) versus those who died unrelated to POEMS syndrome (n = 17) and (B) patients with capillary leak phenotype (n = 19) versus all other patients with known cause of death (n = 30).
Of the 32 patients who died related to POEMS syndrome or treatment complications, the most common cause was a capillary leak phenotype (n = 19, see below), followed by active treatment complications (n = 5), late therapy complications (n = 5), and other POEMS related causes (n = 3). The active therapy complications included a bacterial pneumonia, a COVID infection-related death, a sudden death at home 115 days post-autologous stem cell transplant, and a peri-autologous stem cell transplant death characterized by a protracted course including engraftment syndrome, C. difficile colitis, CMV viremia, pancytopenia, esophageal candidiasis, bacteremia, and possible autologous graft-versus-host disease of the colon. The delayed treatment complications as primary cause of death included secondary acute leukemia in 3 and secondary myelodysplastic syndrome in 2. Another 2 patients had early secondary MDS but were classified as death due to CLP and treatment complications because they had active POEMS at their time of death.
The 3 patients who died related to POEMS but did not fit in any of the other 2 categories included one patient who died of complications of non-cirrhotic portal hypertension with varices and two patients who died while on or shortly after discontinuing POEMS-directed therapy due to cachexia and/or decision to enter hospice. Their respective ages at time of death were 61, 76, and 79 years. The liver biopsy of the patient who died of complications of non-cirrhotic portal hypertension with varices only revealed nodular regenerative hyperplasia without fibrosis or cirrhosis. Her serum ascites albumin gradient was elevated.
Capillary leak phenotype (CLP)Uncontrolled terminal CLP was observed in 19 patients and was the most common cause of death in our cohort. It was characterized by a course of unrelenting ascites, effusions, and/or anasarca that ultimately resulted in hypotension, and cardiopulmonary failure. Median time from terminal CLP to death was 4 months. Terminal CLP was part of POEMS syndrome presentation for 6 patients. In contrast for the remainder, CLP occurred much later in the patients’ course including 5 patients who developed terminal CLP more than 5 years after POEMS diagnosis (Table 2). Median time to death from POEMS diagnosis for patients succumbing to CLP was 2.5 years (95% CI 0.6, 4.1), Fig. 2b. The only notable differences between those patients who died of uncontrolled CLP versus death due to all other known causes were that the CLP group was diagnosed more recently (median diagnosis year 2007 versus 2002, p = 0.02), they were younger at time of death (62 versus 65 years), had higher diagnostic platelet counts (469 × 106/mL versus 415 × 106/mL, p = 0.04), and were more likely to have had ascites at POEMS presentation (53% versus 17%, p = 0.01), Table 3. They were also less likely to have received ASCT (26% versus 58%, p = 0.03).
Table 2 Treatment course among patients dying of uncontrolled capillary leak phenotype (CLP).Table 3 Baseline characteristics by whether capillary leak phenotype was cause of death.Eleven of the 19 patients with terminal CLP had complete medical records available during the treatment of the terminal CLP event. A hallmark feature that this cohort shared was overt anasarca and volume overload without a clear explanation. Common causes of ascites and effusions were evaluated and excluded including cardiac and liver dysfunction (Table 4). Six of 7 patients who underwent echocardiogram during an episode of capillary leak had elevated RVSP (range 40 to 67 mmHg) consistent with pulmonary hypertension with intact left ventricular ejection fraction (range 50% to 69%). Two patients underwent right heart catheterization or Swan-Gantz catheter measurements. Hemodynamic studies showed significant pulmonary hypertension for both patients with pulmonary artery systolic pressure of 59 and 84 mmHg (normal <20 mmHg). Both patients had normal cardiac output with a cardiac index of 2.5 and 3.67 L/min/m2 further supporting that cardiac dysfunction was not the underlying etiology of the volume overload.
Table 4 Patient characteristics during terminal episode of capillary leak phenotype.Liver dysfunction was considered given the presence of anasarca, ascites, and hypotension, but patients had no evidence of liver nodularity on available imaging or other sequelae of cirrhosis such as esophageal or gastric varices. Peritoneal fluid analysis and serum-ascites albumin gradient (SAAG) were inconsistent. Three patients had SAAG less than 1.1 which would indicate non-portal hypertension, while 3 had SAAG greater than 1.1. No patient met criteria for spontaneous bacterial peritonitis at the time of paracentesis. The ascites was often refractory to diuretic management and 8 patients required repeated paracentesis for symptomatic management.
Seven patients experienced shock requiring intravenous vasopressors. Shock was distributive in nature with severe peripheral vasodilation, hypotension and end-organ hypoperfusion, apart from one patient who had obstructive shock caused by cardiac tamponade requiring emergent pericardiocentesis. Other causes of distributive shock such as sepsis, adrenal crisis, and drug reactions were ruled out.
Only after developing anasarca, refractory ascites, and pleural effusions, did these patients experience progressive renal failure. Median creatinine during an episode of capillary leak was 2.1 mg/dL. Only one patient had evidence of nephrotic range proteinuria. No patient had a light chain cast nephropathy phenotype. Diuresis was typically unsuccessful, and 6 patients required hemodialysis for both volume removal and renal clearance. Dialysis presented another challenge as it was commonly poorly tolerated due to hypotension. Renal pathology was available for two patients and both showed thrombotic microangiopathy.
VEGF levels during the terminal episode of CLP were measured in 11 patients with median level of 257 pg/dL (range 63.2–1785; normal range <96.2 pg/mL). Median IL-6 level for the 4 patients with measurements was 20.6 pg/mL (range 3.1–36.76; normal range 0.31–5 pg/mL).
An assortment of therapies were unsuccessful in treating the CLP including alkylators, corticosteroids, immune modulator drugs, anti-CD38 antibodies, and anti-VEGF antibodies (Table 2). While most therapies were ineffective at treating CLP, two patients stand out because they had prior episodes of capillary leak symptoms which were responsive to anti-plasma cell therapy. Patient ID#18 had an 11.3-year course prior to his third and terminal episode of CLP. At initial presentation, he was hospitalized for anasarca, neuropathy, and 15 kg weight loss, and was found to have restrictive lung disease with severely reduced FEV1 and FVC. He was started on plasma exchange without improvement, followed by radiation therapy to a biopsy-indeterminate T8 lesion. Radiation was terminated after 5 of planned 22 fractions due to worsening respiratory failure. He ultimately required vasopressor support and tracheostomy placement for refractory respiratory failure. Symptoms improved after initiation of combined high-dose corticosteroids and cyclophosphamide, which he continued for a total of 17 months followed by prednisone alone for an additional 24 months. He was able to return to work full time and was treatment-free for nearly 4 years, but he again developed anasarca and respiratory failure. He responded well to bortezomib and dexamethasone both with a reduction in VEGF levels (213 to 44 pg/mL) after 3 cycles and improvement in his ECOG performance status from 3 to 1. Further bortezomib was held for worsening neuropathy, and he underwent ASCT. He clinically improved for another 4 years, but once again relapsed with CLP. This was further complicated by an underlying myelodysplastic neoplasm (del(5)(q13q33)). VEGF level increased from undetectable to 87 pg/mL, and he had worsening anasarca, ascites, profound weakness, hypotension, respiratory failure and renal failure requiring dialysis. Velcade was recommended and he was treated locally without further follow-up at Mayo Clinic. He died shortly thereafter.
The other patient (ID#10) had CLP as a presenting feature two years prior to official POEMS syndrome diagnosis and the terminal episode of CLP. He had diffuse anasarca, large-volume ascites, pleural effusion, and subacute renal failure (creatinine rise from 1.4 mg/dL to 3.8 mg/dL). These symptoms initially resolved with prednisone treatment alone as the diagnosis of POEMS syndrome was not initially recognized. Upon prednisone taper, symptoms recurred with worsening renal function and anasarca. After 22 months of prednisone therapy, he was brought to the hospital in respiratory arrest due to pneumonia. A diagnosis of POEMS syndrome was made, and he was started on thalidomide but this was discontinued within one month due to worsening neuropathy. Cyclophosphamide was initiated, but had no effect on the anasarca, pleural effusions, ascites requiring frequent paracentesis, and severe weakness. He developed multisystem organ failure including respiratory failure requiring intubation with subsequent tracheostomy, hypotension requiring vasopressors, and renal failure requiring dialysis. He died ultimately from cardiac arrest after 3 months of complicated hospitalization.
留言 (0)