
記住我

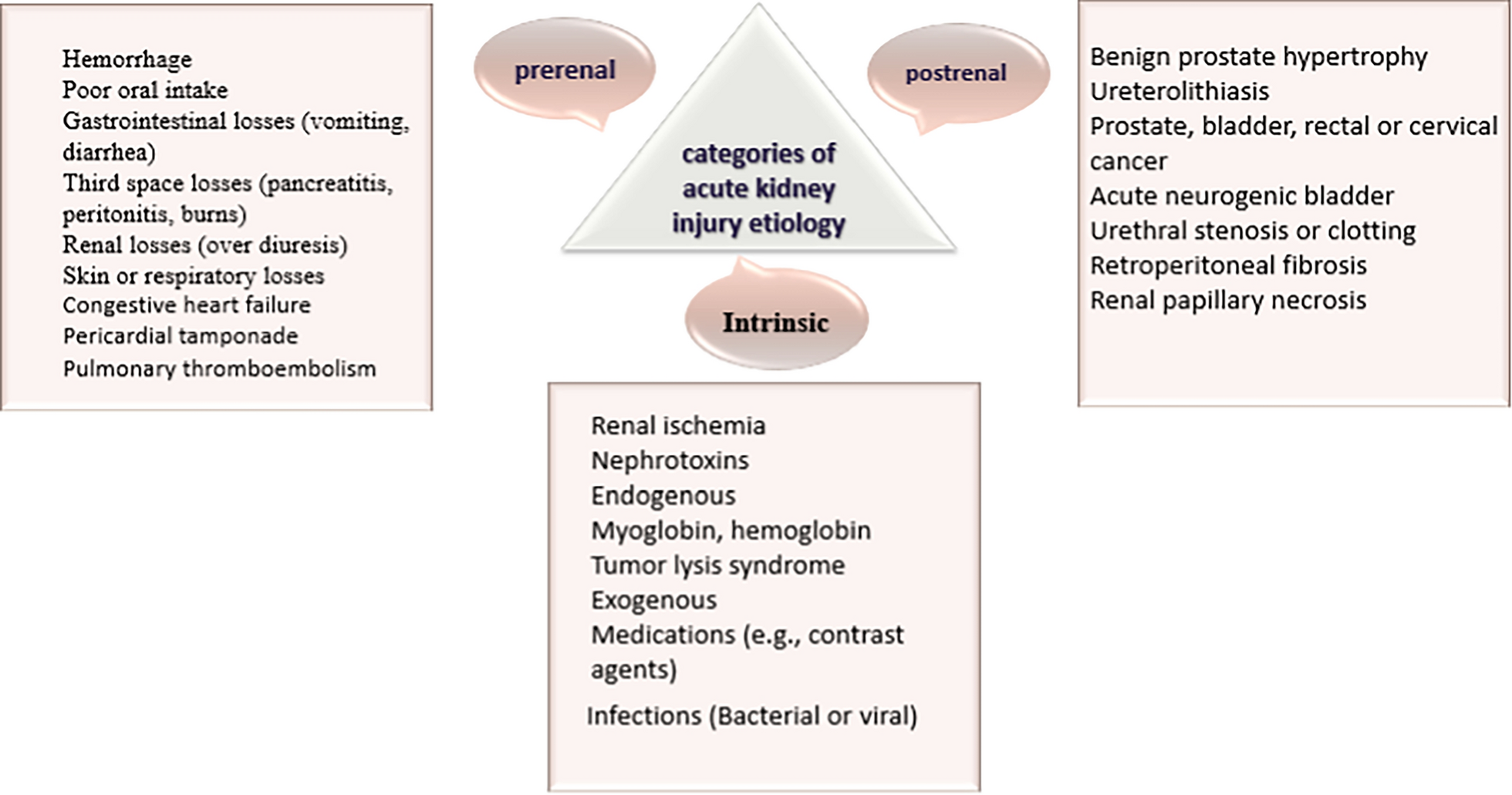



AKI due to BKPyV infection affects up to 10% of transplant recipients. BK nephropathy usually develops early post-transplant, often within the first year, and is driven by persistent high-level viral replication in an immunosuppressed environment [39]. The presence of BKPyV in KTRs most often induces UTIs which is the most common cause of AKI in KTRs [40]. In the case of kidney transplantation, BKPyV infection occurs in the transplanted kidney, and in other organs such as heart, liver, and lung [6]. Also, tubulointerstitial nephritis (TIN) happens when an immune-mediated infiltration of the kidney, causes inflammation and leads to kidney injury [41]. BKPyV causes tubulointerstitial nephritis, which leads to AKI and ureteral obstruction [4]. This review will describe the possible pathways that BKPyV reactivation triggers to produce AKI in KTRs, summarized in Fig. 2.
Fig. 2
The possible ways that BKPyV reactivation can cause AKI in KTRs
Signaling pathwaysSignaling pathways such as NF-κβ and TGF-β signaling can play important roles in BKPyV activity and the occurrence of AKI, which are discussed below.
NF-κβ signalingThe activation of NF-κB during viral infections is seen as a defensive mechanism against viruses and is characteristic of most viral infections because it enhances the expression of numerous proteins involved in both innate and adaptive immunity [42]. In some cases, viral molecules efficiently bind to receptors to trigger a signaling cascade that activates NF-κβ. In other cases, the activation of dsRNA-dependent protein kinase (PKR), which engages with the IKK complex via its catalytic domain and interacts with viral products like dsRNA and viral proteins, triggers NF-κB activation [42].
Once NF-κβ is activated, it triggers the production of antiviral substances such as type I IFNs and proinflammatory cytokines [43] through myeloid differentiation primary response 88 (MyD88) or TIR-domain-containing adapter-inducing interferon-β (TRIF) signaling pathways [44].
NF-κB is crucial as it enhances the production of chemokines, cytokines, adhesion molecules, and enzymes responsible for generating secondary inflammatory mediators [45] and, it is closely linked to the onset of AKI [46]. Studies demonstrate that NF-κB is downregulated by KIM-1-mediated epithelial cell phagocytosis, which can protect the kidney after ischemia- and cisplatin-induced AKI [47].
During AKI, NF-κB can induce an increase in the infiltration of M1 macrophages into the kidneys and cause more damage. In animal models, Mice are protected from kidney injury due to reduced NF-κβ activation, which leads to decreased cell death and chemokine expression (48). Hence, BKPyV infection can activate NF-κB which is one of the most important components of AKI pathogenesis, and can lead to major signaling pathways that involve mostly in inflammation (Fig. 3).
Fig. 3
Activation of NF-κβ during BKPyV infection triggers the production of antiviral molecules such as type I IFNs and proinflammatory cytokines like TNF-α which causes an elevation in apo-A4 levels during AKI, that results in aggravated inflammation and harm to the kidney. This process also, induces an increase in the infiltration of M1 macrophages into the kidneys by NF-κβ activation that can cause more damages
TGF-β signalingTGF-β is produced by a variety of cells, including kidney cells, where BKPyV reactivates. Immunosuppressive medications taken by KTRs increase the activity of TGF-β [49]. Likewise, TGF-β enhances the BKPyV gene's activity, contributing to its replication and subsequent reactivation in KTRs [49]. Researches revealed that when cells from individuals with BKPyV virus were activated, they produced IL-10 and TGF-β [50]. As well, inhibition of UL16-binding protein 3 (ULBP3) by BKPyV, leads to the production of TGF-β in infected cells, which then interferes with the functioning of NK cells [51].
All three isoforms of TGF-β bind to the type II TGF-β receptor, a serine/threonine kinase. Upon binding of the ligand, the type II receptor forms a heterodimer with the transforming growth factor-β type I receptor (TGFβRI), leading to the activation of Smad-dependent and independent pathways such as MAPK and GTPases, which subsequently modify gene expression. TGF-β is a crucial profibrotic growth factor that becomes activated in AKI [52].
In conclusion, BKPyV virus causes acute kidney injury through the upregulation of TGF-β, which leads to renal fibrosis and inflammation. BKPyV has been shown to enhance the activity of TGF-β, promoting its replication and reactivation within KTRs. As TGF-Beta levels rise due to BKPyV infection, the delicate balance of kidney function is disrupted. cells infected with BKPyV produce high levels of TGF-β, which can interfere with the functioning of NK cells. This interference, along with the inhibition of ULBP3 by BKPyV, leads to further upregulation of TGF-β and exacerbates kidney injury. Smad3, a key mediator of TGF-β signaling, plays a pathogenic role in renal inflammation and fibrosis [53]. Its interaction with cyclin-dependent kinase inhibitors (CDKIs) such as p21 and p27 can trigger tubular epithelial cell death by causing G1 cell-cycle arrest. This process is crucial in the pathogenesis of AKI as it triggers cell death pathways [53]. Various activators of TGF-β, such as matrix metalloproteinase and integrins, are upregulated in AKI, leading to increased TGF-β activation and subsequent tissue damage. The TGF-β signaling pathways play a role in sustaining damage to the proximal tubule by encouraging de-differentiation, cell cycle arrest, and heightened vulnerability to apoptosis. Moreover, TGF-β signaling is involved in macrophage chemotaxis, endothelial injury, and myofibroblast differentiation following AKI [54] (Fig. 4).
Fig. 4
BKPyV upregulates TGF-β; Smad3, an essential mediator of TGF-β signaling, promotes the expression of CDKIs like p21 and p27, leading to tubular epithelial cell death through G1 cell-cycle arrest which significantly contributes to AKI by activating cell death pathways
Inflammatory mediatorsNumerous cytokines secreted by leukocytes and renal tubular cells within the damaged kidney are crucial factors in the onset and advancement of AKI inflammation, as well as contributing to BKPyVAN allograft dysfunction in kidney transplant recipients [55]. Some of the most critical cytokines are discussed below.
TNF-αTNF-α, a multifunctional cytokine, is recognized for its various impacts on the immune system, maintaining a balance between proinflammatory and immunosuppressive effects. It plays a significant role in numerous types of renal inflammatory conditions. Although TNF-α is usually undetectable in normal kidneys, it is generated by most renal cells in the presence of inflammation. Mesangial cells and tubular epithelial cells, as well as epithelial cells and podocytes demonstrates an elevation in TNF-α expression after being exposed to certain danger signals [56].
Human collecting duct epithelial cells (HCDCs) can react to BKPyV infection through the activation of viral receptors like TLR3 and RIG-I. This activation triggers an inflammatory pathway resulting in the production of proinflammatory cytokines and chemokines. These inflammatory mediators, in conjunction with their receptors, play a crucial role in mounting an effective antiviral response. The TNF/TNFR system is often recognized as a key player in this antiviral activity [56].
In KTRs with BKPyV infection, the stimulation of TNF-α contributes to the replication of BKPyV, while the blockade of TNF-α suppresses viral replication, presenting a potential therapeutic approach. These findings imply that neutralizing TNF-α could be a viable clinical strategy for treating BKPyV infection [57].
CD8 + T cells are essential in BKPyV infection, leading to the development of BKPyV-specific T cells in circulation and allograft tissue. Furthermore, the stimulation of VP1 and LT-Ag triggers the activation of numerous immune cells and cytokines, such as TNF-α, as the cascade continues [44]. Oxidative stress plays a significant role in ischemic and cisplatin-induced injuries by activating the NF-κB transcription factor. This activation leads to the production of proinflammatory cytokines, such as TNF-α, which is observed through increased TNF-α mRNA levels in both ischemic and cisplatin-induced renal injuries [58]. TNF-α and its receptors, TNFR1 and TNFR2 exhibit significant expression levels during renal inflammation. Upon activation of TNF-α, TNFR1's intracellular portion interacts with TNF receptor-associated death domain (TRADD), which then recruits additional adaptor proteins [59]. TNF-α triggers an elevation in apo-A4 levels during AKI, resulting in aggravated inflammation and harm to the kidney [60]. A study indicates that both LPS and intravenous TNF can lead to similar renal damage, including ultrastructural changes in the glomerular endothelial fenestrae and extensive modifications in the glomerular endothelial cell surface layer. These alterations increase albumin permeability and reduce GFR. The lack of these changes in the glomerular endothelial structure in LPS-treated Tnfr1 − / − mice, along with maintained GFR, highlights the crucial role of TNF-induced glomerular endothelial damage in LPS-induced AKI and suggests its significant involvement in the development of sepsis-induced AKI [61].
In conclusion, TNF-α plays a critical role in mediating inflammatory responses in the kidney, including in the context of BKPyV-induced AKI.
IL-6Elevated levels of IL-6 and other proinflammatory cytokines were identified in kidney biopsies with BKPyVAN [62]. Moreover, a study indicated that IL-6 in urine rises with a high viral load of BKPyV infection [63]. The upregulation of IL-6 can be the result of TNF-α which has a role in BKPyV infection interacting with its receptors. TNF-α can enhance inflammation in human kidney cells by elevating IL-6 levels and at the same time allows for an amplification of renal tubular response to viral infection [56].
On the other hand, recent research has revealed a strong association between the expression of IL-6 and the occurrence of AKI. During the experimentation on animals with ischemic AKI, it was observed that the transcription and signaling of IL-6 were increased both locally and systemically after 60 min of bilateral kidney ischemia suggesting that the IL-6 signaling pathway has the potential to serve as both a biomarker and a target for therapeutic interventions in ischemic AKI [64]. In cases of nephrotoxin-induced AKI, there is a significant increase in IL-6 expression within the kidney, particularly in the renal TECs. This increase is strongly associated with kidney damage and plays a crucial role in activating neutrophils, which is a key mechanism underlying AKI [64]. Early elevation of urine IL-6 has been observed in patients with AKI. Studies in animals indicate that the inability of proximal tubules to metabolize IL-6 leads to higher levels of IL-6 in both the bloodstream and urine which could potentially contribute to the adverse systemic effects and heightened mortality rates associated with AKI [65].
IL-6 increases DNMT1 levels, leading to the methylation of FOXO3a and subsequent decrease in FOXO3a expression. FOXO3a inhibits the Wnt/β-catenin pathway, thereby mitigating renal fibrosis in AKI. IL-6 promotes renal fibrosis in AKI through the regulation of the DNMT1/FOXO3a/Wnt/β-catenin axis [11], highlighting the intricate role of IL-6 in the pathogenesis of AKI associated with BKPyV infection. The mechanism by which BKPyV leads to AKI through IL-6 is complex and multifaceted. The virus triggers an immune response that results in the release of IL-6, which then causes damage to the kidneys, ultimately resulting in AKI (Fig. 5).
Fig. 5
During BKPyV infection, plenty of immune cells and cytokines are stimulated as the continuum cascades, including TNF-α that can enhance inflammation in human kidney cells by elevating IL-6 levels leading to elevation of DNMT1 to induce FOXO3a methylation and reduces FOXO3a expression. FOXO3a blocks the Wnt/β-catenin pathway to alleviate renal fibrosis in AKI
IL-15The upregulation of IL-15 expression by an infectious agent is essential for the activation of NK cells, CD8 T cells, and other immune system cells, allowing them to effectively eliminate pathogens. The availability of IL-15 can influence both innate and adaptive immune responses. [66]. BKPyV-infected endothelial cells exhibit a decrease in the expression of certain genes associated with the immune defense, such as IL-15, indicating the potential use of strategies by BKPyV to suppress the immune system by inhibiting the activation of genes involved in the anti-viral response[67]. Additionally, apoptosis plays a crucial role in the death of renal epithelial cells (REC) and the loss of function during AKI in various experimental models, such as sepsis, ischemia–reperfusion injury (IRI), cisplatin toxicity, mechanical obstruction, and polycystic disease, exhibit similar apoptotic features including nuclear condensation, caspase activation, DNA fragmentation, guanosine triphosphate (GTP) depletion, mitochondrial dysfunction, and the generation of reactive oxygen species [68]. IL-15's protective effects were shown in three different tests for apoptosis, which show both early and late stages of cell death. Several kidney diseases that progress to fibrosis, including acute interstitial nephritis, IgA nephropathy, and diabetic nephropathy, are also marked by an uneven ratio between IL-15 and TGF-β within the kidneys. Specifically, there is a decreased expression of IL-15 and an elevated expression of TGF-β [67].
In addition to its other functions, IL-15 can also hinder the formation of renal fibrosis. It opposes apoptosis and TGF-β induced-epithelial-mesenchymal transition in primary tubular epithelial cells through autocrine loops and membrane-bound forms. Moreover, IL-15 exhibits a protective effect on the kidneys in multiple in vivo models of acute renal injury by preventing cell death and mitigating inflammation through the inhibition of monocyte chemoattractant protein 1 (MCP-1) expression (69). Reduction of IL-15, along with the decrease in antifibrotic factors like BMP-7 and HGF, may serve as a pivotal event in the pathogenesis of renal fibrogenesis and acute and chronic kidney diseases [70].
the downregulation of IL-15 in AKI caused by the BKPyV can have detrimental effects on kidney function. IL-15 plays a crucial role in protecting the kidneys from apoptosis, inflammation, and fibrosis, and its reduction can contribute to the progression o f AKI to chronic kidney disease. Therefore, the reduction in IL-15 expression as a result of BKPyV infection can cause AKI by increasing apoptosis.
IL-11A recent study has highlighted the roles of IL-6 and IL-11, particularly in the context of inflammatory responses (0, 3, 6, and 9 days post-infection) in the supernatants of the 3D BKPyV cell culture using enzyme‐linked immunosorbent assay (ELISA). Notably, IL‐11 showed a significant increase during infection, making it an interesting therapeutic target. Additionally, treating the infected 3D cultures with a neutralizing IL‐11 antibody resulted in a substantial decrease in BKPyV copy rates in the treated cultures compared to the untreated ones [71].
Stimulation of tubular epithelial cells by IL-11 results in the inactivation of GSK3β through ERK- and p90RSK-mediated pathways, leading to the upregulation of SNAI1 and the expression of pro-inflammatory genes. In mice with AKI, IL-11 is upregulated in tubular epithelial cells, causing an increase in SNAI1 expression and kidney dysfunction. This effect is not observed in IL-11 deleted mice or mice treated with a neutralizing IL-11 antibody in either preemptive or treatment modes. Treatment with anti-IL11 in AKI reduces all pathological manifestations [72].
Upregulation of IL-11 in cells infected with BKPyV triggers the activation of ERK and p90RSK, leading to the phosphorylation of GSK3β at Thr43 and Ser9. This phosphorylation event results in the inactivation of GSK3β, which subsequently inhibits GSK3β-mediated SNAI1 phosphorylation. Consequently, SNAI1 accumulates and suppresses the transcription of its target genes, such as E-Cadherin, potentially contributing to the development of AKI (Fig. 6).
Fig. 6
Elevated IL-11 levels during BKPyV infection lead to increased activity of ERK and p90RSK. This results in GSK3β inactivation by phosphorylation of Thr43 and Ser9. This prevents GSK3β-mediated SNAI1 phosphorylation causing SNAI1 accumulation and the transcriptional suppression of its target genes, prototypically E-Cadherin which can lead to AKI
留言 (0)