Surveillance of influenza samples in Chongqing High-Tech Zone revealed the molecular epidemiological characteristics of influenza virus strains, including detection rates and temporal variations of major genotypes. These findings contribute to understanding influenza virus transmission patterns and trends, support the iterative updating of influenza virus strains, and help predict transmission and pathogenicity, thus providing a scientific basis for public health decision-making [21,22,23,24].
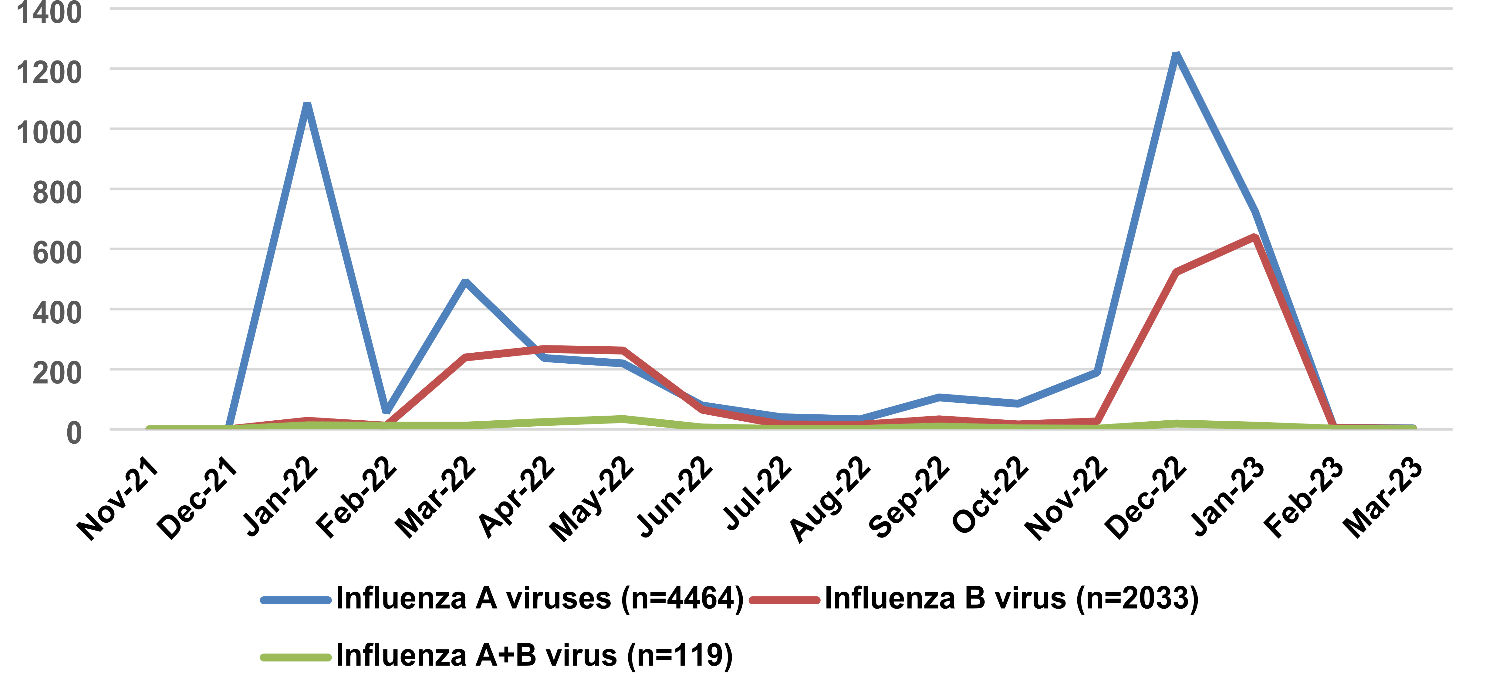
Chongqing Hi-tech Zone has a strong population mobility, which increases the likelihood of influenza generation, prevalence, and dissemination. Therefore, monitoring the pathogenetic and epidemiological patterns of influenza in this area is particularly significant. This study analyzed all ILIs reported at Chongqing Hi-Tech Zone University Hospital from November 2021 to April 2024. Both influenza A and B peaked during the winter and spring seasons, with influenza B peaking later than influenza A. This finding is consistent with previous literature reports [25,26,27]. It can be concluded that influenza A predominantly dominates the epidemic season.
From April 2023 to April 2024, there were 241 positive cases of influenza A and 207 positive cases of influenza B. Among the influenza A cases, H3N2 was the predominant subtype, while Victoria was the main subtype for influenza B. The H1 subtype of influenza A was absent throughout 2023 but accounted for 82% of the cases in January 2024 and 16% in February 2024. The Yamagata subtype of influenza B did not appear from 2023 to 2024 [26]. The study found that children aged 0–10 years were affected by influenza. There was a statistically significant difference in the detection rates of influenza A and B viruses between males and females in this age group (p < 0.05) [28,29,30].
The SAA and CRP levels of 241 influenza A positive cases and 207 influenza B positive cases were analyzed, showing statistically significant differences between the two groups (p = 0.000 for SAA and p = 0.001 for CRP). The CRP levels were 7.9 mg/L in the influenza A positive group and 18.7 mg/L in the influenza B positive group. The SAA levels in the influenza A positive group were significantly higher than in the influenza B positive group. The CRP level in the influenza A positive group was significantly higher than in the influenza B positive group. A correlation was found between influenza A and B positivity and elevated SAA levels, with influenza A positivity showing a stronger correlation with elevated SAA [31,32,33,34].
It was shown that inflammation markers were higher in influenza A than influenza B. Studies have shown that patients infected with influenza A exhibit a more pronounced inflammatory response compared to those with influenza B. For instance, a comparative study of severe and critical influenza B in children highlighted that while both types of influenza can lead to significant morbidity, the inflammatory markers associated with influenza A infections tend to be elevated [35]. Additionally, research on the cellular immunophenotype expression during influenza infections indicated that influenza A is associated with a higher fraction of certain immune cell types, such as CD14 + and CD4 + IL-17 A + cells, compared to influenza B [36].
Moreover, the differential ability of pandemic and seasonal H1N1 influenza A viruses to alter neutrophil function suggests that influenza A may provoke a more robust immune response, potentially leading to increased inflammation [36]. This is further supported by findings that show higher levels of pro-inflammatory cytokines in patients with influenza A, which can contribute to the severity of the disease [37].
In the context of co-infections, it has been observed that influenza A infections are more likely to be complicated by secondary bacterial infections, which can exacerbate the inflammatory response and lead to worse clinical outcomes [38]. The overall immune response to influenza A, characterized by heightened inflammation, underscores the need for vigilant monitoring and management of patients infected with this virus [39].
The correlation between influenza A and B positivity and SAA elevation was notably strong. In summary, winter and spring influenza in Chongqing’s High-Tech Zone is predominantly caused by influenza A, though influenza B is also prevalent. Among the positive cases, H3N2 is the primary subtype for influenza A, while Victoria is the primary subtype for influenza B. Elevated SAA levels are correlated with both influenza A and B positivity.
Furthermore, developing and optimizing influenza prevention and control strategies is crucial for mitigating the impact of seasonal and pandemic influenza. Effective strategies must be informed by robust surveillance systems, vaccination programs, and public health interventions. For instance, the Global Influenza Strategy 2019–2030 emphasizes the need for improved surveillance and vaccination efforts in regions like Latin America and the Caribbean, where seasonal influenza is associated with significant morbidity and mortality [1].
Moreover, the application of mathematical models, such as the moving epidemic method, can help define epidemic thresholds and guide timely interventions. A study conducted in Tunisia demonstrated the utility of this method in determining influenza epidemic and intensity thresholds, which can inform local health authorities about when to implement control measures [2].
In addition to vaccination, nonpharmaceutical interventions play a vital role in controlling influenza transmission. A review of personal protective measures and environmental hygiene in nonhealthcare settings highlighted the importance of hand hygiene and the use of face masks, although evidence from randomized controlled trials suggests limited effectiveness in reducing transmission [3].
Although the study demonstrates the epidemiological characteristics of influenza virus infection and the potential application of inflammatory markers, several limitations exist. The limited sample size may restrict the generalizability of the findings. Additionally, the study did not analyze the effect of different influenza A virus strains on the levels of 14 inflammatory markers or explore the potential influence of other respiratory pathogens on these markers.
Future studies will explore the mechanisms behind these epidemiological features to obtain more comprehensive and objective findings. Additionally, further research is needed on the expression patterns of inflammatory markers in different populations, such as children, the elderly, and patients with chronic diseases, and their role in the preventive mechanisms of influenza vaccination. As research deepens, a clearer understanding of the function and importance of the influenza vaccine and inflammatory markers will provide a solid theoretical basis for influenza prevention and treatment.





留言 (0)