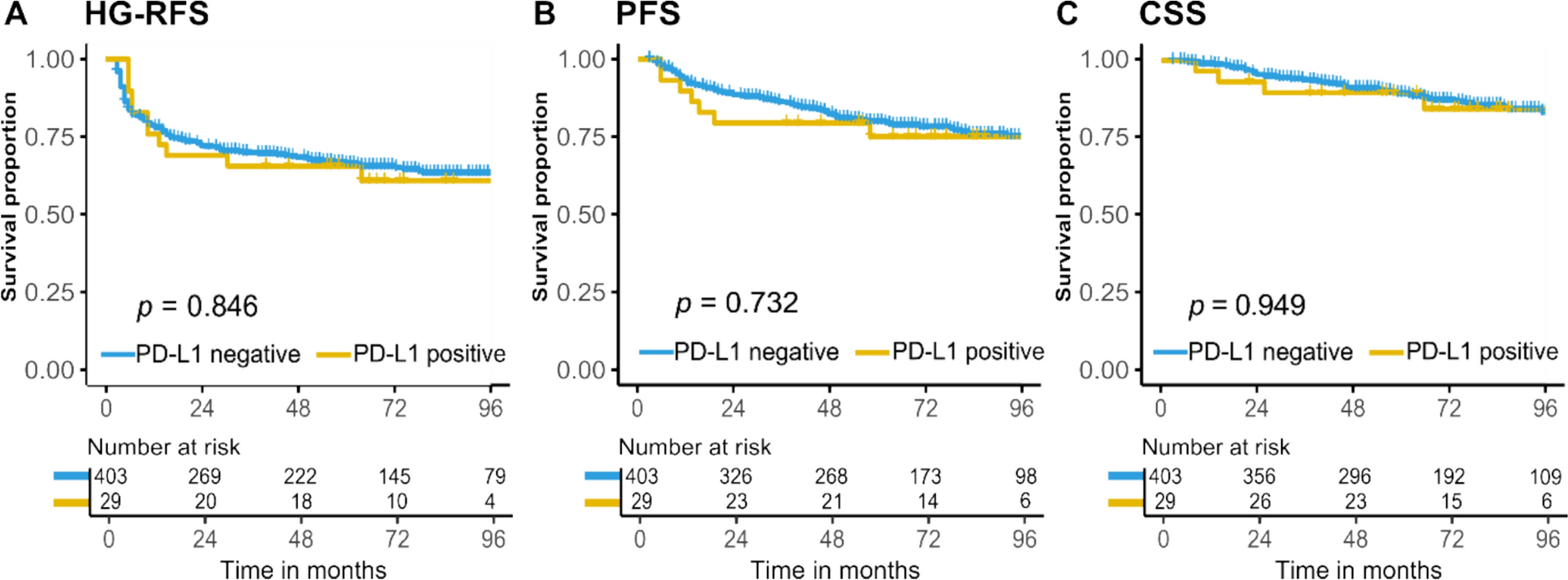
We investigated if PD-L1 protein expression was associated with response to BCG in a large and unbiased cohort of HR-NMIBC patients (N = 432) who received adequate BCG therapy with long-term clinical follow-up. We found that PD-L1 expression was positive in only 7% of tumors, and this expression was not associated with outcomes after BCG treatment in BCG-naïve tumors. Neither a change in the recommended 5% cut-off in tumor-infiltrating ICs nor an investigation of TCs altered these results. In addition, we found that aggressive tumor features were associated with increased PD-L1 expression, consistent with studies showing that PD-L1 overexpression correlates with BC stage progression [8, 9].
Previous studies showed that PD-L1 expression did not correspond with response to BCG, but the study populations consisted of small sample sizes (N = 22 to 186), and in 4/6 studies, varying antibodies were used [16,17,18,19,20,21]. Of particular interest are two studies that provide dissimilar evidence. Pierconti et al., investigated SP142, SP263, and 22C3 PD-L1 mAbs in N = 65 primary CIS patients, of which N = 37 developed HG recurring disease [22]. The percentage of samples that were PD-L1 positive based on tumor and immune cells was similar for SP142 and 22C3. SP263 showed inconsistent staining patterns. Only 22C3 was associated with recurring disease, while SP263 and SP142 did not differ between responders and non-responders, identical to the results presented in this study. A study by Kates et al. in N = 63 BCG-naïve tumors showed that PD-L1 (both 22C3 and SP142), using the combined positive score, was overexpressed in BCG non-responders (N = 32) [23]. Because of the patchy distribution of PD-L1, a whole slide analysis was performed. The percentage of SP142 staining is up to 28%, which could be because investigators used a selected cohort overrepresenting non-responders and a different scoring system. Based on contradictory findings and our study which indicates that PD-L1 expression has no prognostic value, we consider PD-L1 unfit as a biomarker for response to BCG.
We found that patients who recurred more often showed high PD-L1 expression. In 22 BCG-treated NMIBC patients that were sampled pre- and post-BCG, enhanced PD-L1 expression in tumor recurrences was seen, suggesting a PD-L1-mediated resistance mechanism [24]. In contrast, Boorjian et al. showed that patients who received BCG had lower PD-L1 expression at the time of RC, while others found that SP142 was lower in patients with a refractory recurrence [16, 25]. A study of N = 761 urothelial carcinoma patients investigating clinicopathological correlations for SP142 found that no intravesical BCG treatment before PD-L1 testing was associated with positive PD-L1 expression [26]. These findings directly contradict our results, yet multiple caveats must be addressed for the latter studies. The first study included HR-NMIBC patients who had a mixture of primary and recurring disease and not all patients received BCG [25]. In the second study, the mean expression of PD-L1 was generally very low (1.5%), differences were minimal (3% vs 0.6%) and measured in only 14 patients [16]. The third study included nephroureterectomies and stage T2-T4 tumors, which biases the primary analysis, and there was no BCG information given [26]. These caveats make it difficult to draw definitive conclusions.
Beyond its role as a prognostic biomarker, PD-L1 has long been recognized as a therapeutic target. In Keynote-057 (Cohort A, CIS only, N = 101), PD-L1 status was high (38%) in BCG unresponsive patients [12]. Neither the success rate by PD-L1 status nor the specific IHC antibody was mentioned. Considering the low durable response at 3 months from pembrolizumab, the high costs of ICI, other successful and less costly treatments like gemcitabine/docetaxel instillations becoming available and our data showing limited PD-L1 expression (14–25%) in recurring tumors, we argue that PD-L1 monotherapy is not an attractive approach in patients that failed BCG treatment [27]. Preclinical work in syngeneic mice and rats inoculated with BC cell lines and treated with anti-PD-L1 ICI in conjunction with BCG led to a tumor weight reduction and increased cytotoxic T cell immune responses as compared to BCG alone [28, 29]. Studies investigating a combination of PD-1/PD-L1 and BCG seem a more logical way forward. Currently, several of these studies are ongoing (e.g. POTOMAC or CREST). A combination strategy might have the potential to change treatment paradigms if side effects are tolerated.
This study had several limitations. First, we only used the SP142 antibody, while SP142 has shown higher interobserver variability, lower concordance, and lower overall expression as compared to other companion diagnostics [21, 30,31,32]. SP142 should be primarily scored in tumor-infiltrating immune cells and not in tumor cells, which is done in other antibodies and may explain the disparate outcomes. Nonetheless, all studies concluded that SP142 is useful to evaluate PD-L1 status in BC. Plus, the use of a single antibody for all samples prevents antibody-related bias. We found a low prevalence of BCG-naïve cores staining positive for PD-L1, and a potential explanation is that TMAs do not capture the intricate heterogeneity of the tumor microenvironment (TME). Nonetheless, we performed a whole slide analysis with different cut-offs and assessment techniques, but the results remained unaltered. A third limitation was that multiple TMA cores were lost during the production of the TMA, which could have affected endpoint analyses. Albeit we used triplicate cores, we advise using > 1 mm core sizes in the future. Finally, we did not investigate PD-L1 in the context of the TME. Analysis of immune cells such as CD4 + , CD8 + , T regs, and (innate) immune cells might help explain (adaptive) immune resistance mechanisms. Although interesting, this study aimed to assess whether PD-L1 alone could be used as a biomarker for response to BCG treatment.

留言 (0)