
記住我
Overall, 419 mHSPC patients qualified for final analyses, of which 25% (n = 105) received docetaxel vs. 75% (n = 314) ARPI treatment (Suppl. Table 1). Median age at mHSPC was 70 years (IQR: 63–75) with a median PSA of 46 ng/ml (IQR: 13–274). Overall, 4.8% of included patients were classified as ECOG status ≥ 2. Proportions of De Novo, high volume and visceral metastasis at mHSPC were 76%, 64% and 7.8%, respectively. Median follow up was 27 months (IQR: 11–46).
mHSPC: Docetaxel vs. ARPIIn comparison between mHSPC patients treated with either docetaxel vs. ARPI (Suppl. Table 1), patients with ARPI were significantly older at mHSPC diagnosis (71 vs. 66 years), and harbored lower baseline PSA (38 vs. 183 ng/ml, both p ≤ 0.002), relative to docetaxel mHSPC patients. Regarding frailty status, no significant differences in ECOG status distribution, cardiovascular diseases or secondary malignancies were observed (all p ≥ 0.2). MHSPC patients receiving docetaxel harbored significantly higher rates of De Novo (89% vs. 71%), high volume mHSPC (80% vs. 49%) and visceral metastases (15% vs. 5.6%), than ARPI counterparts (all p ≤ 0.01). Regarding treatment responses, lower PSA nadir (0.10 vs. 0.65 ng/ml) and higher ≥ 99% PSA response (70% vs. 54%) were observed for ARPI vs. docetaxel (both p ≤ 0.027).
Regarding cancer-control outcomes, significant differences for all mHSPC patients were observed. Specifically, median time to mCRPC was significantly longer for ARPI than for docetaxel-treated patients (30 vs. 17 months, hazard ratio [HR]: 0.49, p < 0.001, Fig. 2A). In multivariable Cox regression models adjusting for baseline and tumor characteristics, no significant difference remained (HR: 0.96, p = 0.9, Suppl. Table 2A).
Fig. 1
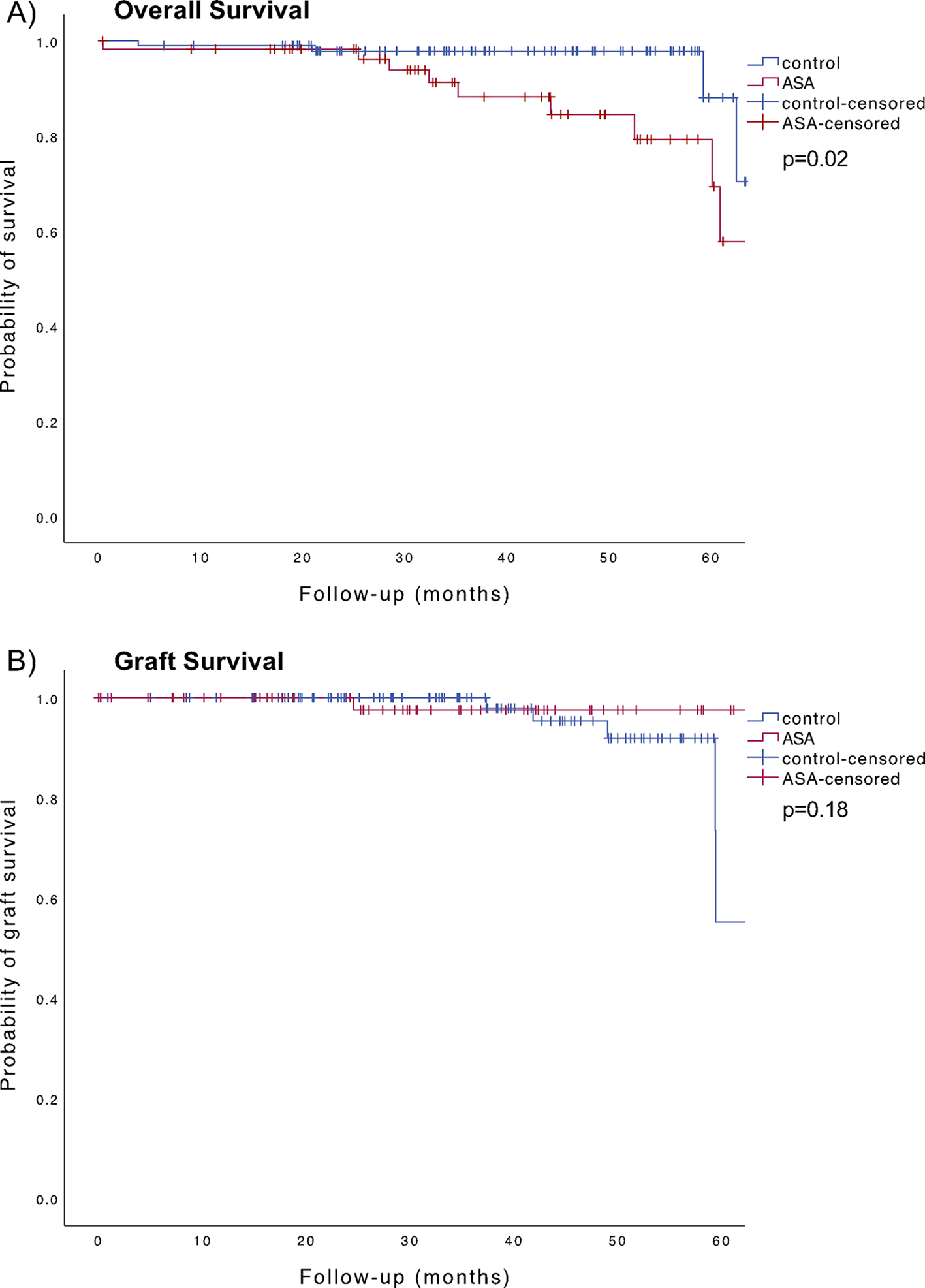
Kaplan Meier curves depicting time to metastatic castration resistant prostate cancer (CRPC, A) and overall survival (B) according treatment for high volume metastatic hormone-sensitive prostate cancer (mHSPC) stratified according to docetaxel vs. androgen receptor pathway inhibitor (ARPI)
In OS analyses, ARPI patients also exhibited significantly longer OS, relative to docetaxel patients (96 vs. 50 months, HR: 0.67, p = 0.03, Fig. 1B). After multivariable adjustment in Cox regression models, also no difference between both treatments remained (HR: 1.03, p = 0.9, Suppl. Table 2B).
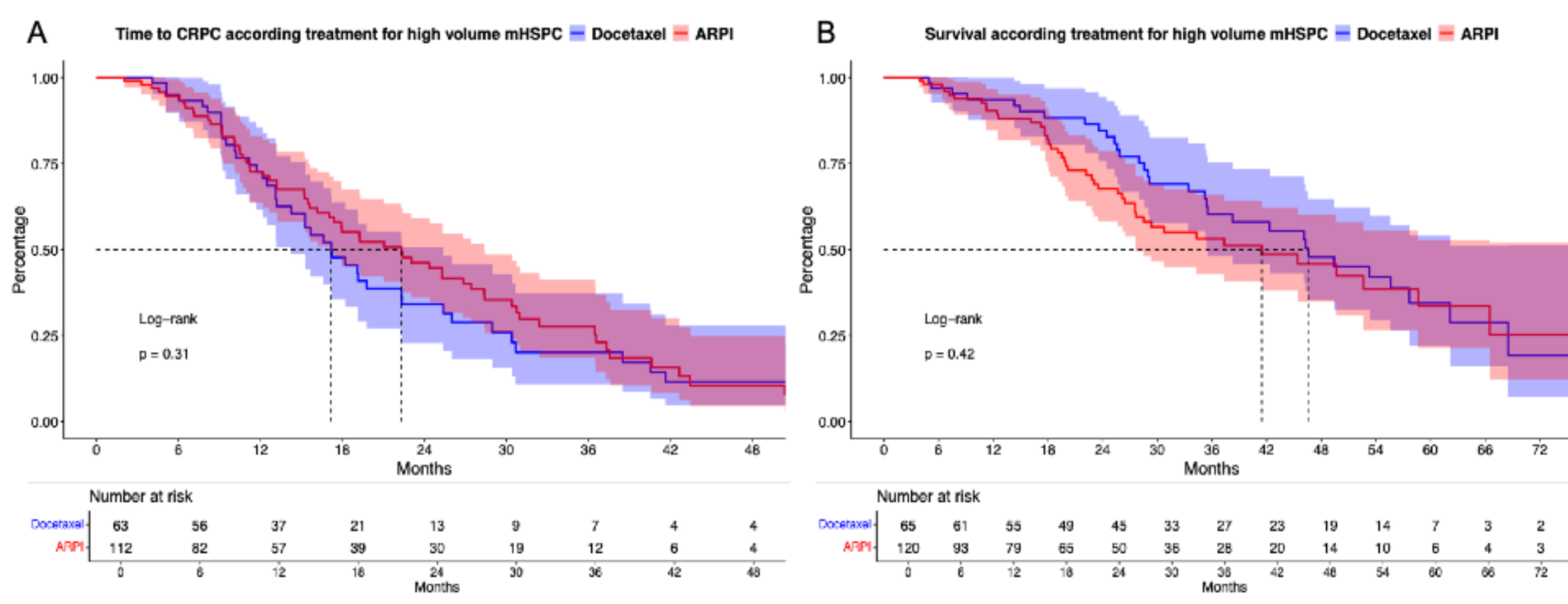
Fig. 2
Kaplan Meier curves depicting time to metastatic castration resistant prostate cancer (CRPC, A) and overall survival (B) according treatment for metastatic hormone-sensitive prostate cancer (mHSPC) stratified according to docetaxel vs. androgen receptor pathway inhibitor (ARPI)
High volume mHSPC: Docetaxel vs. ARPIIn sensitivity analyses of 192 high volume mHSPC patients, 34% (n = 65) received docetaxel vs. 66% (n = 127) ARPI treatment. Patients with ARPI were significantly older in median at mHSPC (72 vs. 67 years) and harbored lower baseline PSA (133 vs. 360 ng/ml, both p < 0.05). No difference in ECOG status distribution, cardiovascular diseases or secondary malignancy rates were observed (all p ≥ 0.12). Moreover, no difference in PSA nadir at mHSPC (0.54 vs. 0.88 ng/ml) or PSA ≥ 99% responses (64% vs. 60%) were observed for ARPI vs. docetaxel (both p ≥ 0.3). Additionally, no differences in rates of De Novo mHSPC (85% vs. 91%) or visceral metastasis (11 vs. 20%) were seen (both ≥ 0.1).
In time to mCRPC analyses (Fig. 2A), no significant difference between ARPI vs. docetaxel high volume mHSPC patients were observed (median time: 22 vs. 17 months, HR: 0.82, p = 0.3). Similarly in OS analyses (Fig. 2B), also no difference between ARPI and docetaxel were observed (median time: 42 vs. 46 months, HR: 1.21, p = 0.4). In both multivariable Cox regression models, no significant differences between both treatments could be computed (Suppl. Table 2A-B).
Sequential therapies for mHSPC and first-line mCRPCSequential treatment information for 143 mHSPC with subsequent progress to mCRPC were available. Of these, 35% (n = 50) received ARPI-ARPI vs. 27% (n = 38) ARPI-docetaxel vs. 38% (n = 55) docetaxel-ARPI combination.
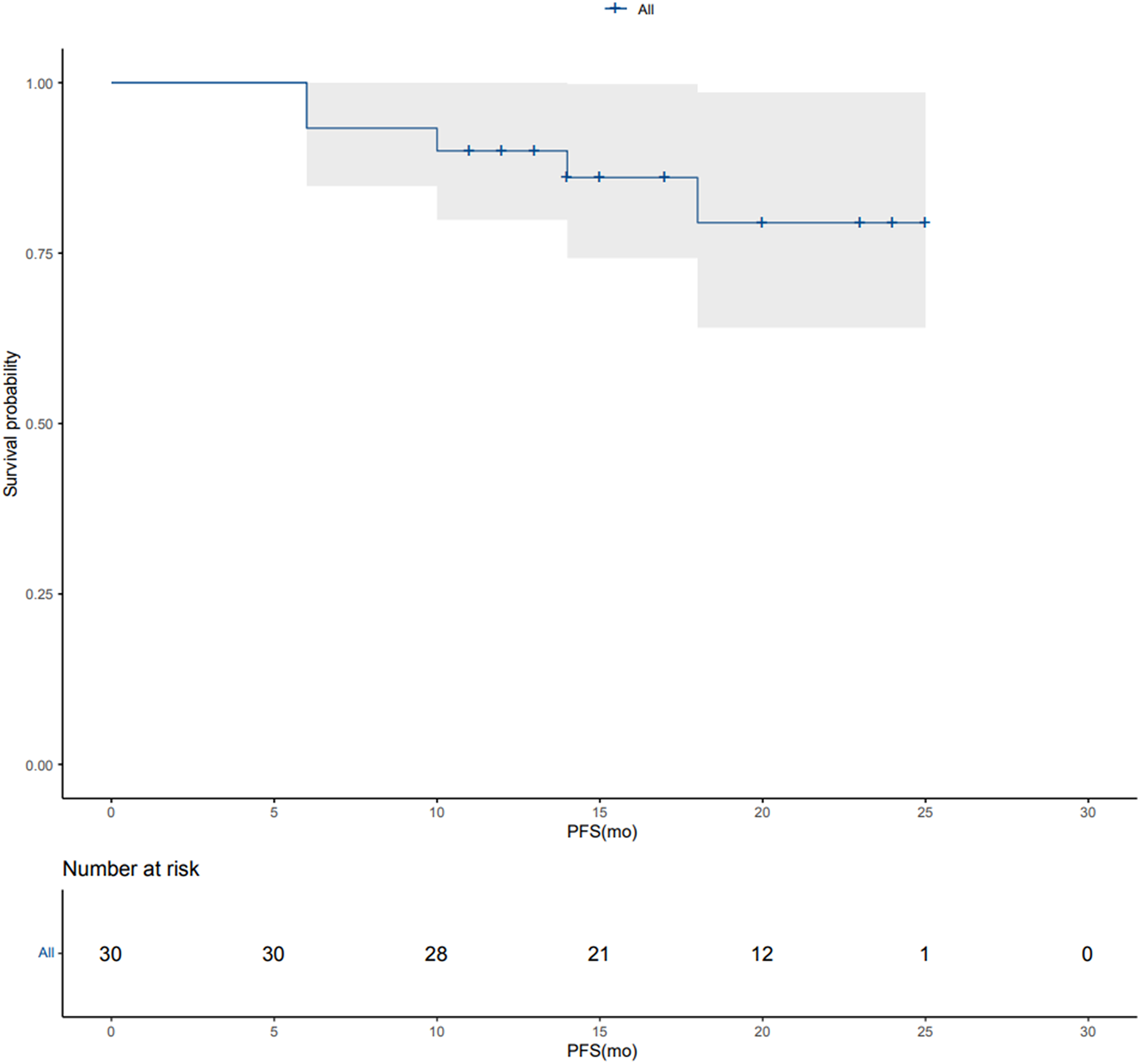
In PFS analysis from time point of progressing to mCRPC (first-line therapy for mCRPC), no significant differences for all three sequential therapies were observed with median time of 10.3 vs. 7.1 vs. 9.2 months for ARPI-ARPI vs. ARPI-docetaxel vs. docetaxel-ARPI combination (Suppl. Figure 1 A, p = 0.3). However, PFS2 was better for ARPI-ARPI over ARPI-docetaxel and docetaxel-ARPI after multivariable adjustment.
In OS analyses (Suppl. Figure 1B), no differences were observed with median OS of 67 vs. not reached vs. 57 months for ARPI-ARPI vs. ARPI-docetaxel vs. docetaxel-ARPI combination (p = 0.5). In landmark-analyses from time point of progressing to mCRPC (Suppl. Figure 1 C), also no OS differences were observed (p = 0.7). In all multivariable Cox regression models, no significant difference between all three compared sequential therapies were observed (Suppl. Table 2 C-D),
In subsequent sensitivity analyses of high volume mHSPC patients (Suppl. Figure 2 A-C), 67 patients qualified for analyses, of which 30% (n = 20) vs. 25% (n = 17) vs. 45% (n = 30) received ARPI-ARPI vs. ARPI-docetaxel vs. docetaxel-ARPI combination. Similar to all mHSPC patients, in high volume mHSPC no differences in PFS for first-line mCRPC treatment and OS analyses were observed for all three compared sequential therapies (all p ≥ 0.3). Finally in multivariable Cox regression models, no significant differences between all three sequential therapies were computed (Suppl. Table 2 C-D).
留言 (0)