Identifying optimal candidates for active surveillance in low-grade intermediate-risk non-muscle invasive bladder cancer
Objective
The intermediate-risk non-muscle invasive bladder cancer (IR-NMIBC) prognostic group is heterogeneous. Growing evidence supports the role of active surveillance (AS) for patients with low-risk NMIBC, however, no clear data exists considering IR-NMIBC. The aim of the study was to assess the risk of recurrence of patients eligible for AS based on the International Bladder Cancer Group (IBCG) stratification.
Methods
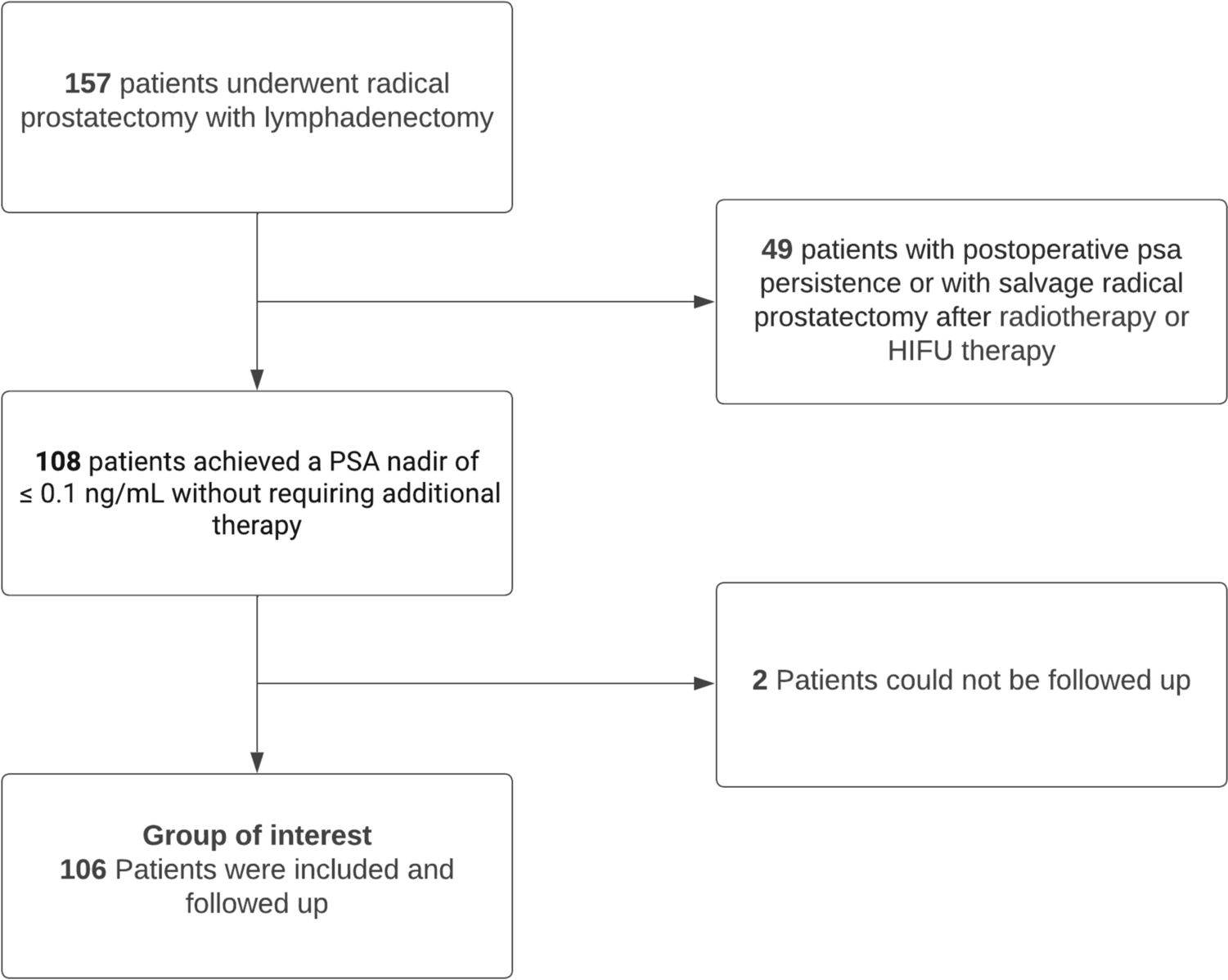
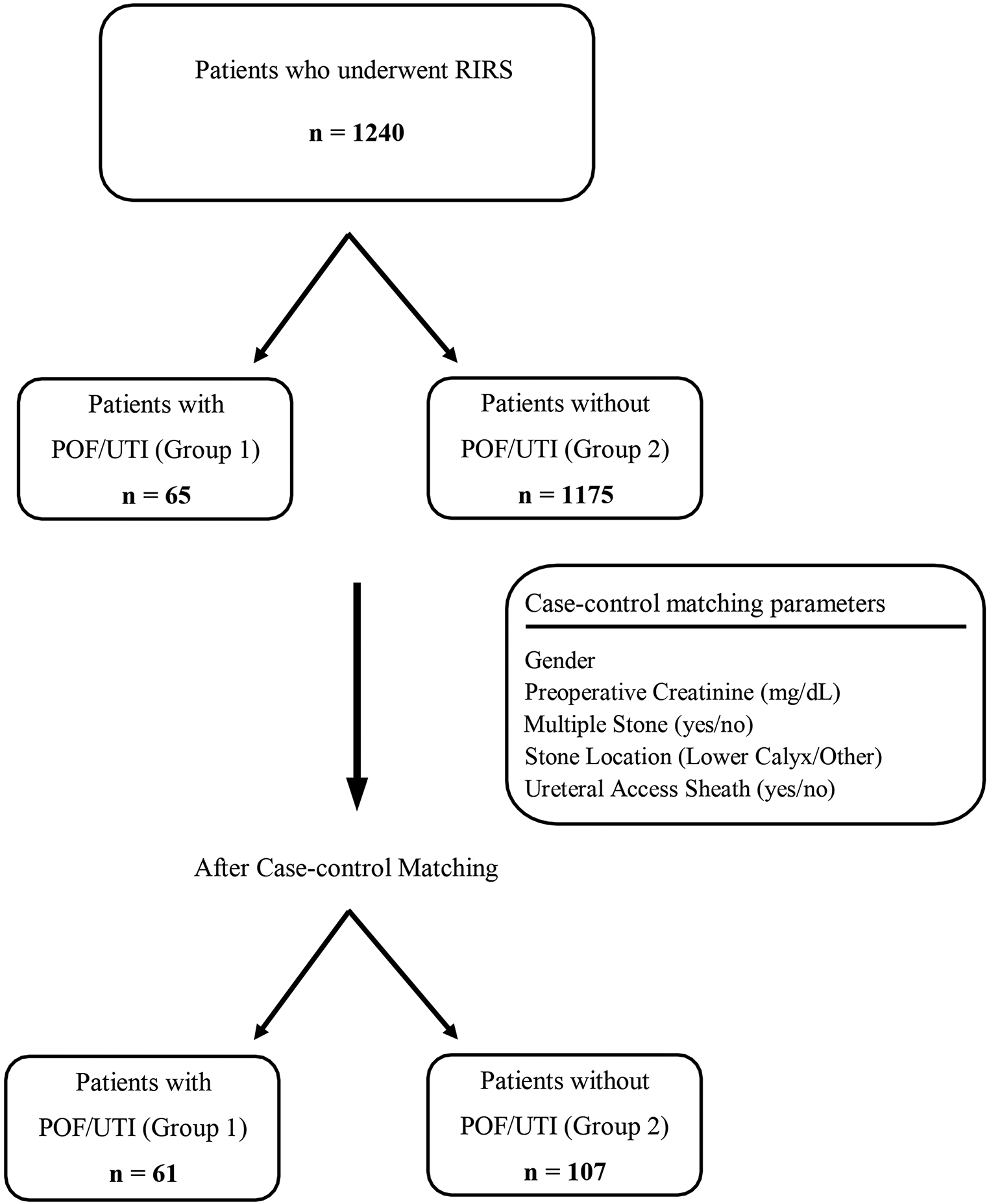
We retrospectively evaluated 174 LG IR-NMIBC patients who underwent transurethral resection of bladder tumor (index TURBT) from 2012 to 2023 at a tertiary referral center and fulfilled the inclusion criteria for enrollment in AS protocols at the index TURBT (≤ 5 suspicious lesions, no macrohematuria, negative urine cytology, lesions ≤ 1 cm). Patients were then stratified according to the International Bladder Cancer Group (IBCG) risk factors: frequent recurrence, early recurrence, previous instillation, and multifocality. Kaplan Meier plots and multivariable Cox regression analysis (MVA) were used to assess the risk of any and high-grade (HG) recurrence according to the number of risk factors.
Results
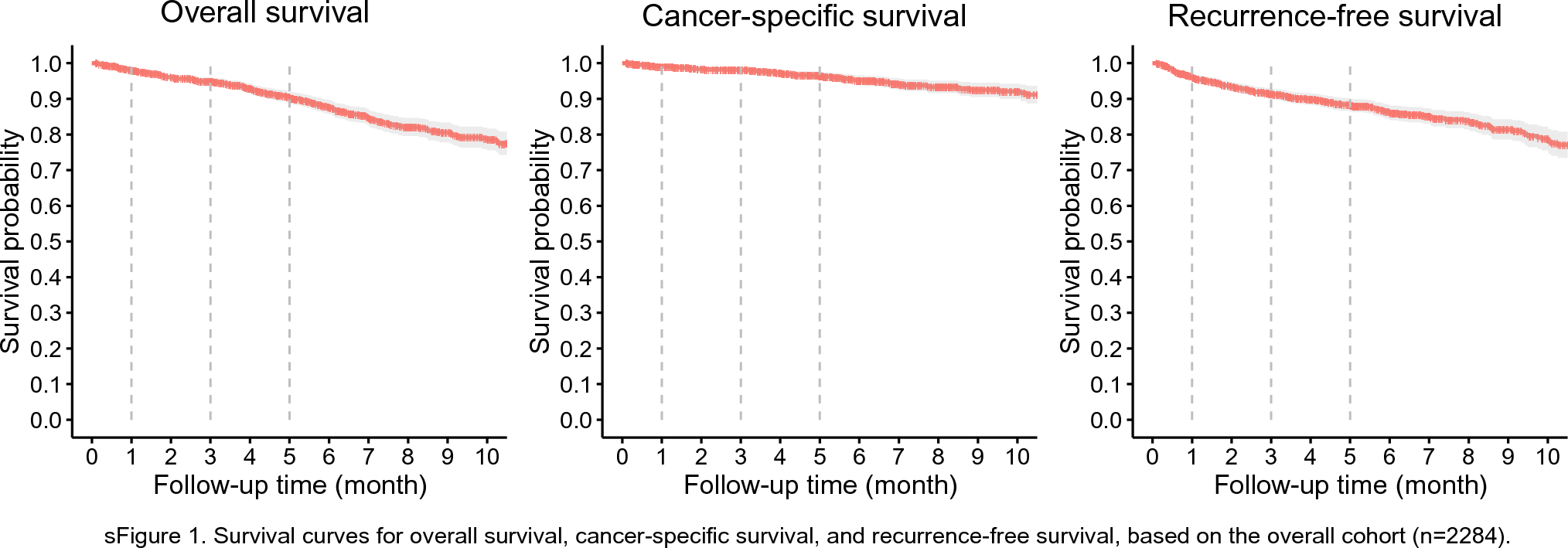
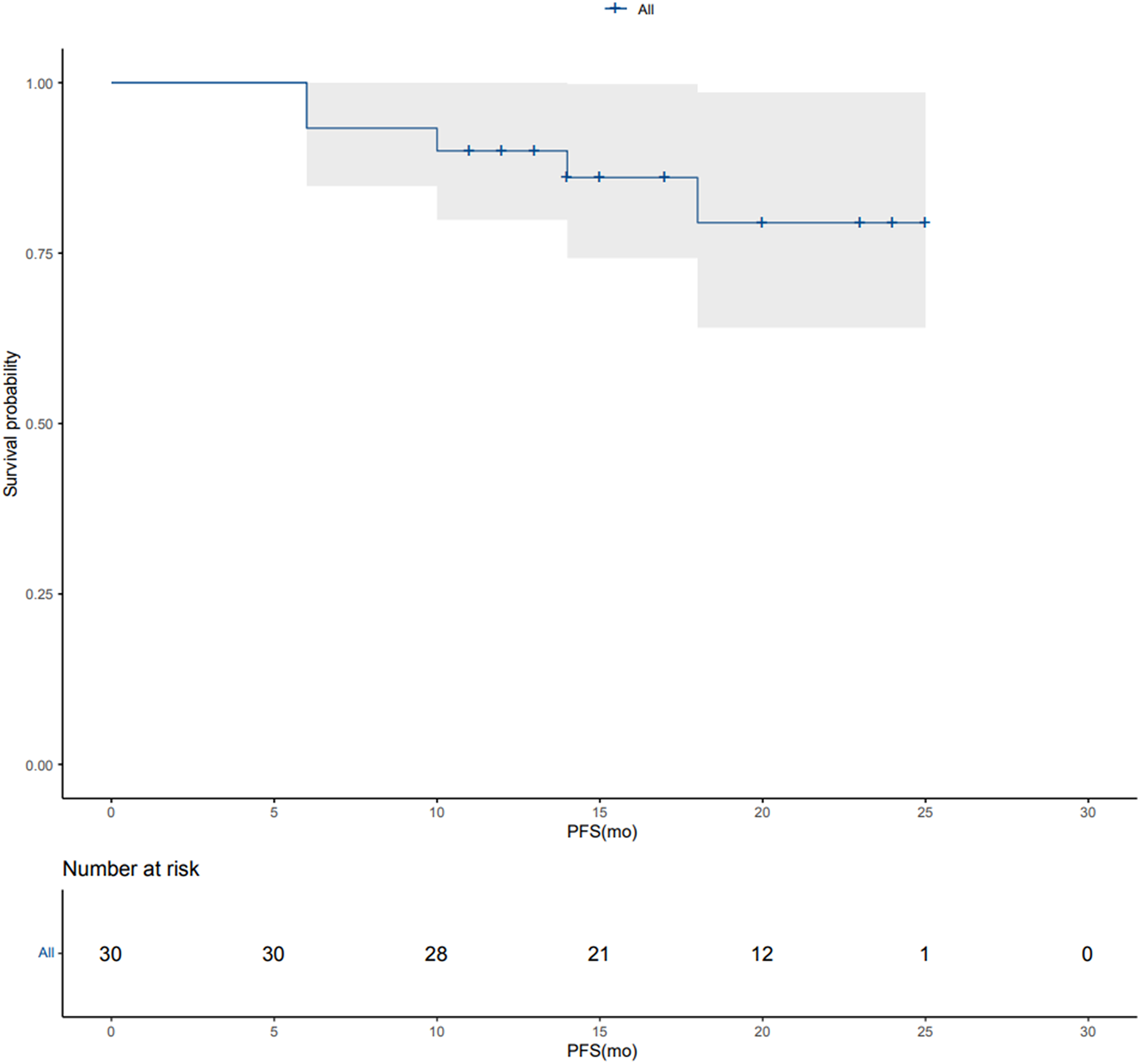
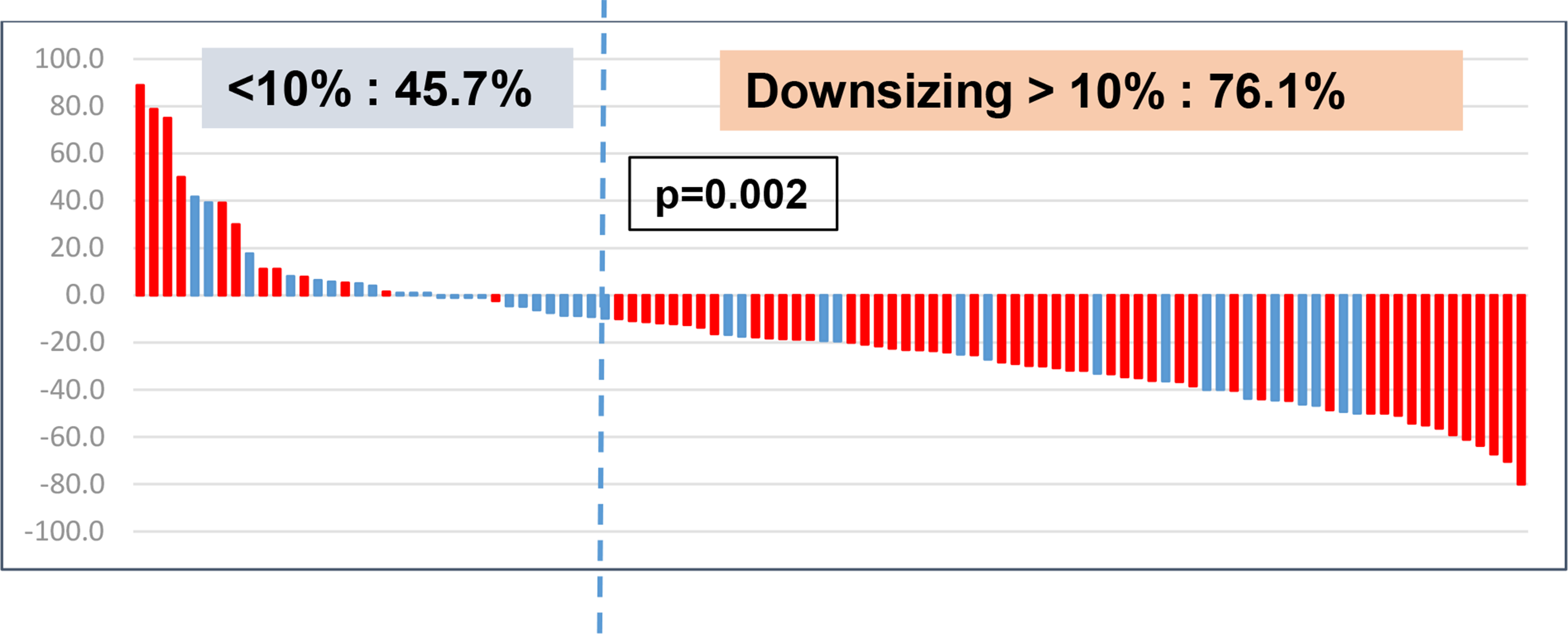
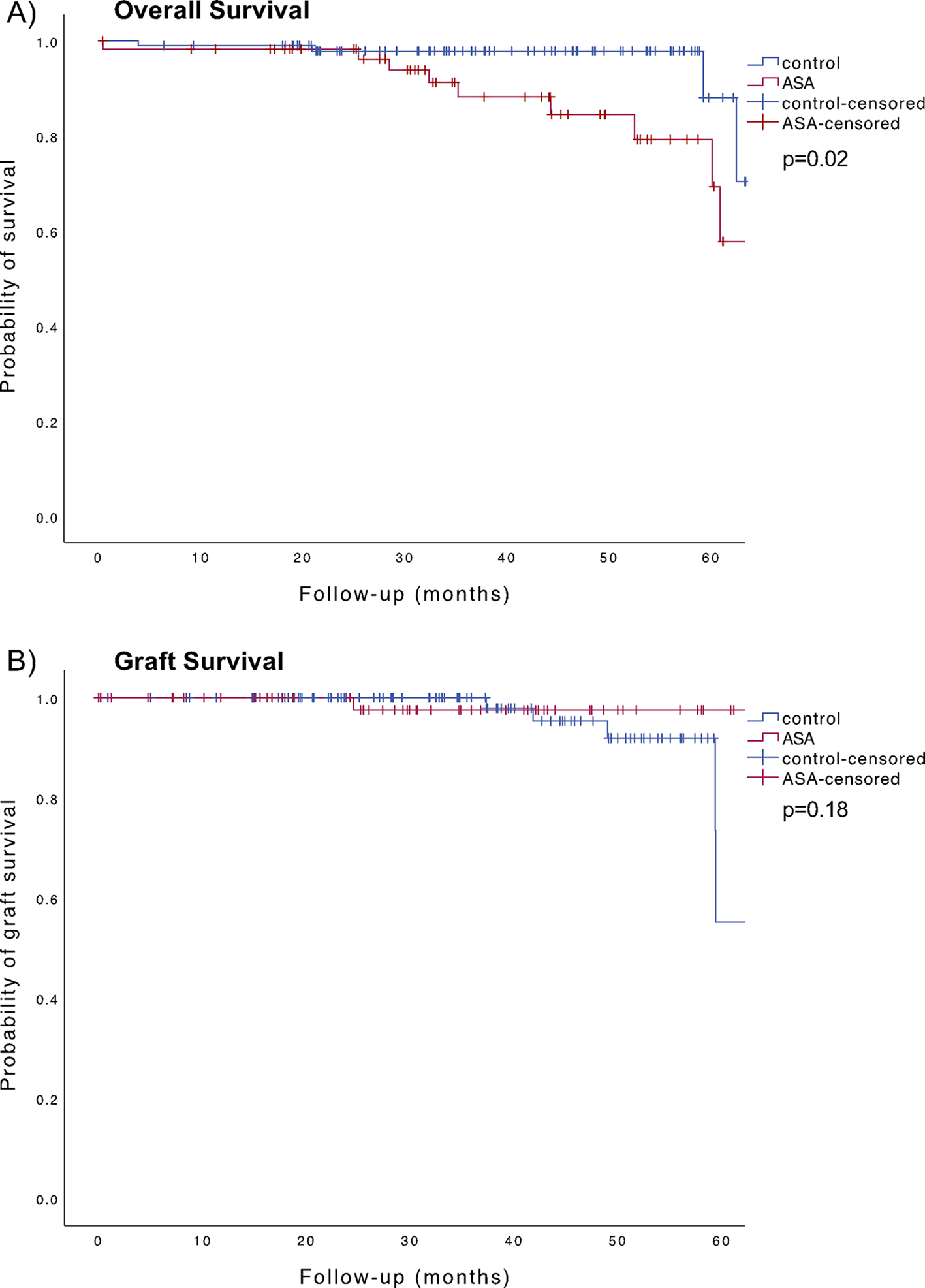
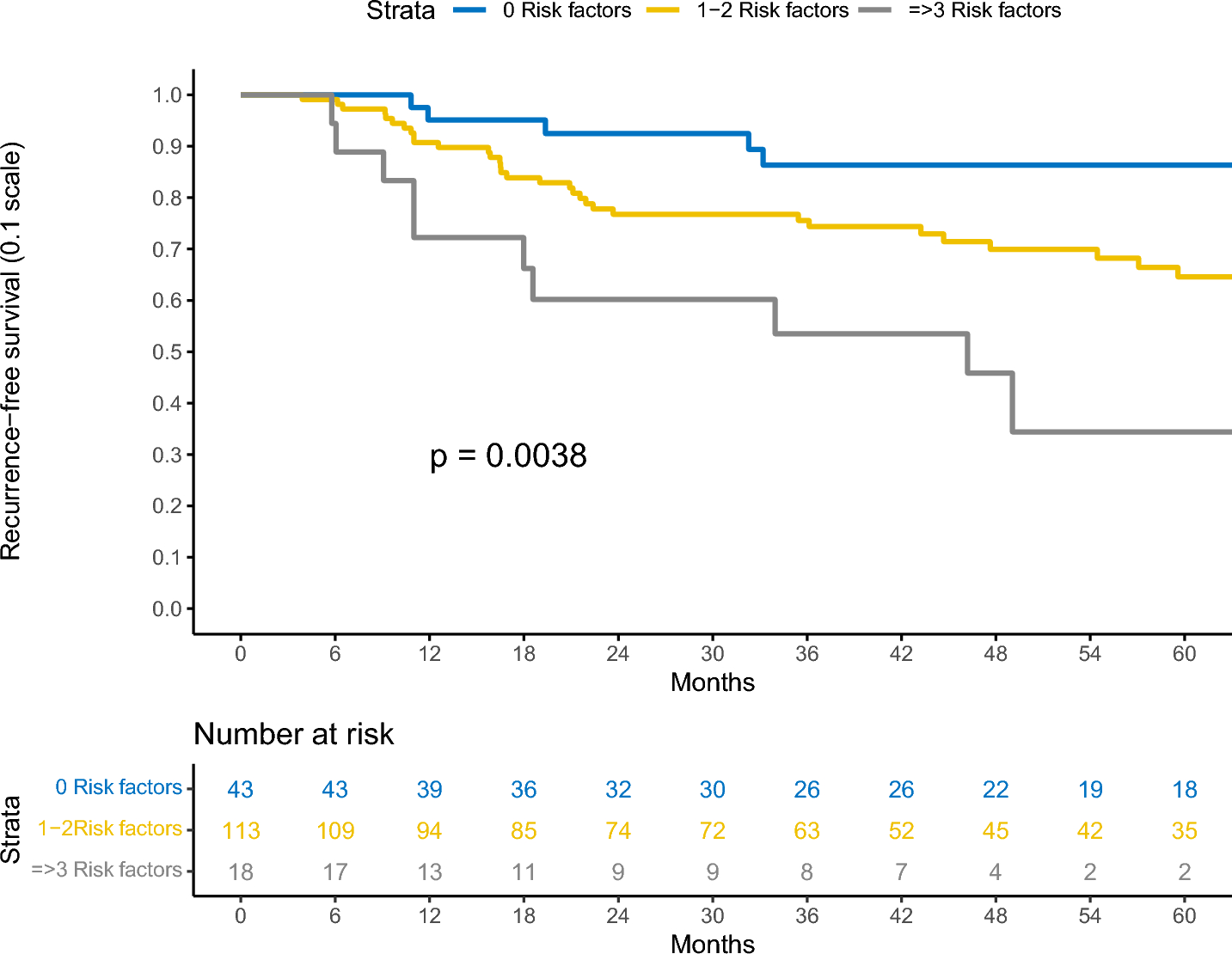
Overall, 168 (97%) patients had a Ta low grade bladder tumor. After a median follow-up of 36 months [Interquartile range (IQR) 20–54], 75 (43%) and 32 (18%) patients experienced any- and HG recurrence, respectively. The 3-year recurrence free-survival (RFS) was 86% [95% Confidence Interval (CI) 76–98%] for patients with 0, 76% (95% CI 68–84%) for those with 1–2, and 54% (95% CI 34–84%) for those with ≥ 3 risk factors. The 3-year HG-RFS was > 90% for patients with 0 and 1–2 risk factors, compared to 76% (95% CI 58–99%) for those with ≥ 3 risk factors. At MVA, the presence of ≥ 3 risk factors was associated with a higher risk of recurrence [hazard ratio: 4.74, 95% CI 1.75–12.8, p = 0.002].
Conclusion
Among patients with LG IR-NMIBC eligible for AS, those with more than 2 IBCG risk factors may not be suitable candidates due to a higher risk of developing HG recurrence. Randomized controlled trials with standardized AS protocols are necessary to validate these findings and optimize patient selection for AS in LG IR-NMIBC.

留言 (0)