Medications that affect blood coagulation, such as AT, are a critical component to consider in the clinical man-agement of patients undergoing KTX, requiring a delicate balance between minimizing thrombotic risk and mit-igating bleeding complications. This retrospective analysis aimed to provide a comprehensive evaluation of the impact of ASA monotherapy on perioperative bleeding in KTRs. Cadaveric donors for Group A were seven years older compared to Group B, reflecting the fact that a substantial number of patients in the ASA group were part of the ESP and therefore part of a more vulnerable KTX sub-cohort. Concordantly, Group A had a higher incidence of CAD, confirming the clinical rationale for ASA use in patients with cardiovascular comorbidities [9]. Key findings indicated that perioperative Hb-loss and intraoperative bleeding rates were not significantly different between both groups, and the incidence of postoperative bleeding indicated by sonographically detected hematomas did not differ (28.8% vs. 26.6%, p = 0.75). However, intraoperative bleeding (15.3% vs. 8.2%, p = 0.17) and the postoperative transfusion rate (22% vs. 13.3%, p = 0.15) were observed to be higher in the ASA group, although not statistically significant. This finding potentially reflects the cumulative effects of the intraoperative bleeding tendencies, which could lead to ongoing minor bleeding. The lack of significant differences in hemoglobin levels between the groups may be attributed to the limited sample size and the administration of erythrocyte concentrates in Group A, which likely contributed to aligning hemoglobin levels between the groups.
Consistent with our findings, Benkö et al. reported a prevalence of bleeding events in the same range, affecting 31.5% of their AT cohort [7]. In contrast, Eng et al. reported a higher transfusion rate of 28.8% in their cohort with preoperative ASA use, but, consistent with our results, did not show a significant difference compared with their control [1]. However, the ASA cohort of Eng et al. showed a 3-fold risk for reoperation, which is not reflected in our results with similar revision rates of 16.9% and 17.1%, respectively (p = 0.95) [1, 7]. Therefore, our results are consistent with those of Musetti et al., who showed an association of AT with a higher transfusion rate, but not with major bleeding events, and concluded that AT should not be considered a contraindication to KTX due to bleeding risk in itself [10]. Nevertheless, the need for close monitoring in cases of minor bleeding that may require transfusion is strongly emphasized in this patient group.
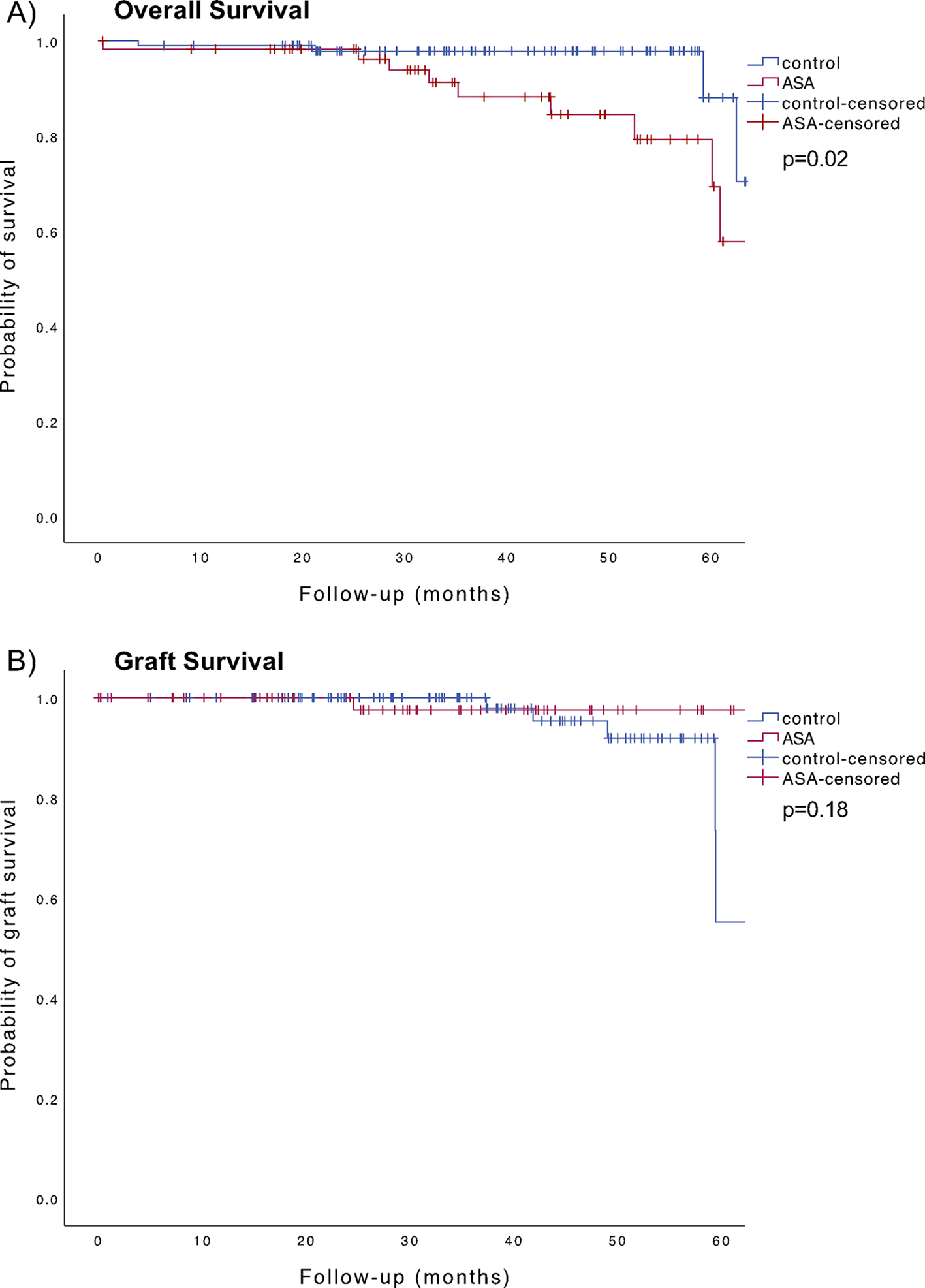
The vulnerability of our cohort is also highlighted by the results regarding the distribution of complications with fewer patients in the ASA group without complications (5.4% vs. 43%), and more patients with CDC Grade 4 and 5 complications (p = 0.01). It should be noted that, by indication for ASA, significantly more patients in Group A had CAD. In addition, angiopathies and infections as underlying ESRD were more common, and the predisposition to infection may be exacerbated by the need for immunosuppression. It is well known that cardiovascular disease and infections are major risk factors for severe complications and death after KTX [11, 12]. Accordingly, the severe complications and the significantly inferior OS of the ASA group must be seen primarily in the context of the underlying comorbidities and cannot be attributed to ASA use directly. This is validated by the results of our study, which indicate that nearly 50% of deaths in Group A were attributable to infections. It is noteworthy that only one death in Group A was related to a cardiac event, which appears low in comparison to the substantial number of CAD patients. Although a significant difference in OS was observed in our study, no significant difference in graft survival was found between the groups, with a tendency in favor of the ASA group in the Kaplan-Meier analysis. Therefore, our findings corrobate the results of the meta-analysis by Cheungpasitporn et al., who demonstrated that ASA use in KTRs is associated with a reduced risk of major cardiac events and appears to be protective against graft failure [6, 13].
Our analysis has several limitations. The retrospective design and single-center setting limit the generalizability. The study’s sample size, though moderate, may still be insufficient to detect small but clinically significant differences in rare outcomes. Moreover, the specific indications for ASA use were not determined in our study.

留言 (0)