
記住我





The choice of comparators in this study, involving alpha-tACS, tDCS, and sham stimulation, is grounded in the need to comprehensively evaluate the efficacy of tES protocols in preventing POD. Alpha-tACS and tDCS were selected based on their demonstrated potential in modulating brain activity, which is crucial to address the pathophysiological mechanisms underlying POD.
The alpha-tACS intervention was chosen based on the previously described disrupted neural network connectivity in the alpha range associated with POD [36].
tDCS applies a constant electrical current, which can modulate neuronal excitability and has been shown to reduce postoperative pain and the POD incidence when applied postoperatively [35].
The sham stimulation serves as the control condition. The sham procedure mimics the application of the active interventions without delivering the electrical current, ensuring that participants, care providers, and outcome assessors are blinded to the intervention.
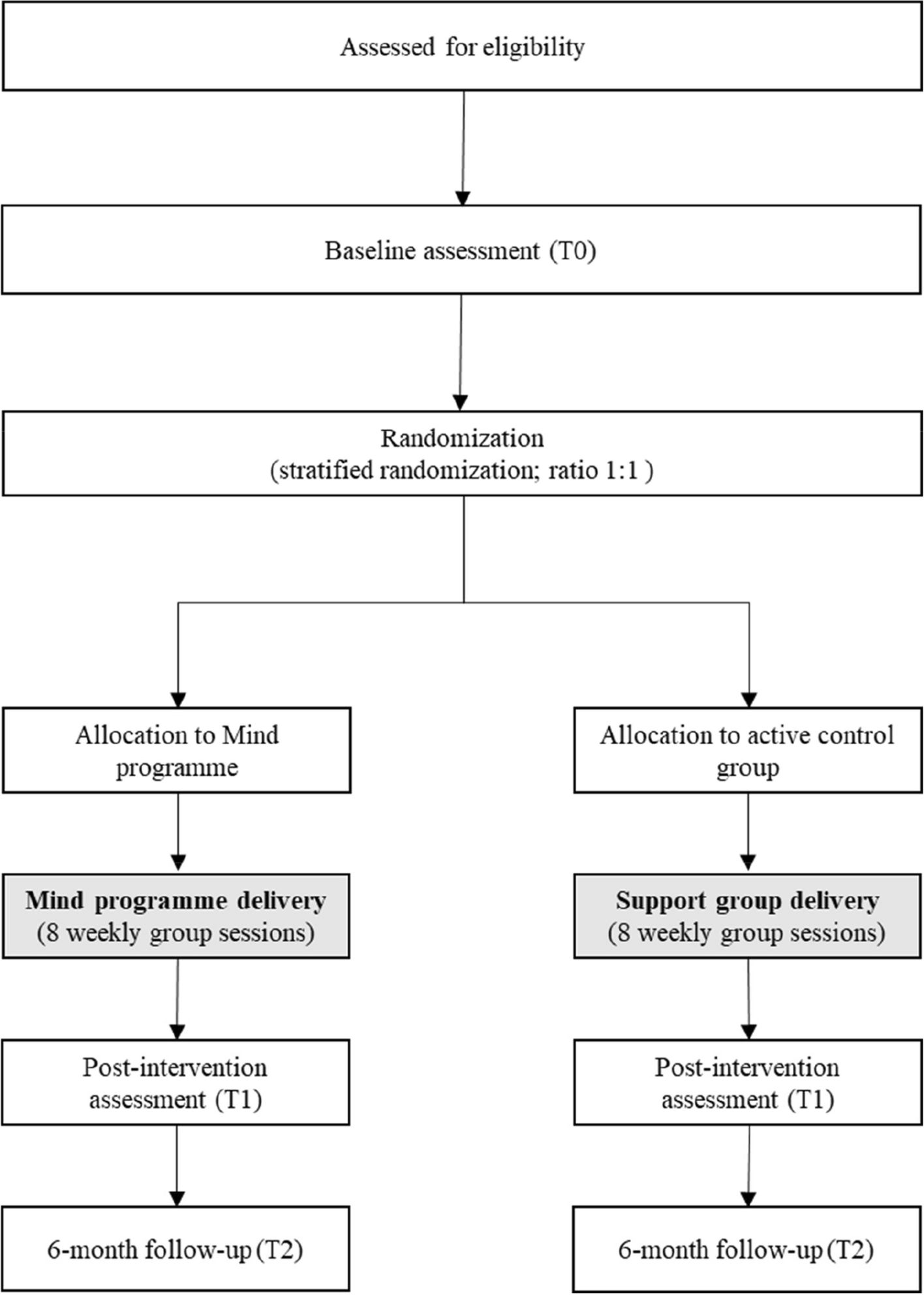
Intervention descriptionPatients will be enrolled at least 1 day before surgery. Questionnaires regarding contraindications for tES as well as baseline questionnaires will be handed out (PPI, HADS, STAI, PCS, BRI, PSQ, DN4). The preoperative cognitive status will be assessed with a MoCA score.
On the day of the surgery, a 64-channel EEG will be recorded in the preoperative holding area. Preoperative delirium and pain will be assessed with standardized tests (RASS, 3D-CAM, and NRS). A preoperative blood sample will be drawn. Before induction of anesthesia, a frontal EEG recording will be started that will last until the end of anesthesia.
A single tES intervention will take place postoperatively in the PACU, after return of consciousness and patient handover to the PACU staff. Emergence of delirium in the PACU (PACU-D) will be assessed, and patients will be asked about postoperative nausea and vomiting (PONV) as well as pain using standardized tests (RASS, 3D-CAM, and NRS) every 30 min for 1 h in the post-anesthesia care unit (PACU). A 64-channel EEG will be recorded, and a second blood sample will be drawn after the tES intervention.
During the first 5 postoperative days, patients will be screened twice daily for POD and pain using standardized tests (RASS, 3D-CAM, and NRS). A third blood sample will be drawn on the second postoperative day (Fig. 1).
Fig. 1
Timeline of the study interventions and visits. PACU post-anesthesia care unit, EEG electroencephalography, tES transcranial electrical stimulation, RASS Richmond Agitation-Sedation Scale, 3D-CAM 3-min diagnostic interview Confusion Assessment Method, NRS Numerical Rating Scale
Baseline questionnairesA questionnaire regarding contraindications for the application of tES will be filled out by the physician enrolling the patient. It comprises questions regarding presence of metallic implants, history of neurosurgical intervention, traumatic brain injury or epileptic seizures, known dermatological disorders, ongoing long-term medication, possibility of a pregnancy, and previous tES application.
A set of questionnaires regarding pain (NRS, DN4), attitude towards pain (PCS, PSQ), and affective disorders (HASD, STAI) will be explained and handed out to the patient.
The Montreal Cognitive Assessment (MoCA) score evaluates cognitive functioning in areas such as attention, memory, language, and visuospatial skills. It will be conducted and scored by a trained study personnel.
EEGA 5-min resting-state EEG with eyes closed will be recorded preoperatively in the holding area and post-intervention in the PACU. EEG data will be recorded using ANT Neuro’s dry EEG system, equipped with dry surface electrodes that do not require the use of conductive gel or paste. This system is designed for a rapid setup, allowing for signal acquisition in this clinical setup. Patients will be lying in bed, and the dry EEG cap, fitted with 64 electrodes according to the 10–20 international system, will be placed on their head. The electrode positions will be adjusted to ensure optimal scalp contact. Patients will be asked to remain still and relaxed, with eyes closed during the recording session of 5 min. Data acquisition will be conducted at a sampling rate of 1064 Hz. The impendences will be monitored and maintained below an ideal threshold of 5 kΩ if possible or the recommended threshold of 100 kΩ.
Intraoperatively, a frontal EEG will be recorded with a common neuromonitoring tool available at the study site (SedLine® Brain Function Monitor by Masimo or Narcotrend®-Compact M by Narcotrend-Gruppe). Both medical devices are used to monitor the brain function of patients under anesthesia or sedation in critical care settings, utilizing raw and quantitative EEG parameters to provide a real-time dimensionless index of sedation depth. Before the start of the recording the study staff ensures the proper functioning of the monitor. For the SedLine Monitor, we will make sure that the feed speed is set at 30 mm/s and the amplitude at 5 mV, since the display settings affect the sampling frequency of the recorded data stored [37].
InterventionThe tES will be administered using a battery-powered stimulator (Neuroelectrics® Starstim Home Research Kit, Barcelona, Spain) via two electrodes (5 cm in diameter) soaked with 0.9% NaCl solution and mounted in a neoprene cap.
To ensure blinding to the stimulation group, the ECG monitoring in the PACU will be masked before the start of the intervention with a stencil covering the raw ECG traces.
In the tACS group, two electrodes will be placed at the P3 and P4 positions of the 10–20 EEG system, over the respective left and right posterior parietal cortex (PPC) (Fig. 2B). A 20-min oscillating stimulation with 2 mA (peak-to-peak) at an age-adapted frequency of 9.5 Hz will be applied. An age-adapted stimulation frequency was determined for this cohort by analyzing a database of 532 clinical resting-state physiological EEG recordings. The method was described in detail elsewhere [38]. In the tDCS group, the anode will be placed over the left DLPFC, as determined by the F3 position of the 10–20 EEG system. The cathode will be placed over the right supraorbital area, corresponding to Fp2 of the 10–20 system (Fig. 2A). The 20-min continuous stimulation with 2 mA will gradually increase and decrease at the beginning and end within an additional 10-s period (ramp time).
Fig. 2
Illustration of electrode placement and electric field distribution. Applied transcranial electrical stimulation on an MNI head/brain for (A) tACS group (stimulation frequency: 9.5 Hz; electrodes centered over P3 and P4; electrode diameter: 5 cm) and (B) tDCS group (electrodes centered over F3, anode, and Fp2, cathode; electrode diameter: 5 cm), simulated using SimNibs [58, 59]. tACS transcranial alternating current stimulation, tDCS transcranial direct current stimulation
The sham group is divided into two subgroups with n(tDCS)/2 for tDCS-sham and n(tACS)/2 for tACS-sham. In these subgroups, the same electrode arrangements and ramp times are used, but the current is only applied for 30 s to induce the typical tingling sensation on the scalp and blind the patients to the stimulation condition.
The perception of side effects associated with the stimulation and group affiliation is surveyed at the end of each stimulation condition using a standardized questionnaire [27].
Blood samplesThree blood samples will be taken for the study: one preoperatively, one postoperatively in the PACU, and one on the second postoperative day, with 5 mL of serum collected each time. The blood samples will be sent immediately after collection to the Greifswald University Hospital biobank for aliquoting and storing. The following parameters will then be determined from these samples in the neurology research laboratory of the Greifswald University Hospital: VILIP-1, CCL2 (MCP-1), sTREM-2, BDNF, TGF-β1, VEGF, IL-6, sTREM-1, β-NGF, IL-18, TNF-α, sRAGE, CX3CL1, CRP, NfL, S100b, VCAM-1, ECAM-1. The samples will be destroyed after measurement.
Postoperative visitsThe RASS, the 3D-CAM, and the NRS score will be assessed once preoperatively in the holding area, every 30 min for 1 h in the PACU (3 times in total) as well as twice a day for 5 days postoperatively.
The Richmond Agitation-Sedation Scale (RASS) score is a commonly used tool to assess a patient’s level of agitation or sedation, ranging from + 4 (combative) to − 5 (unarousable), with 0 representing an alert and calm state [39]. Patients with a postoperative RASS score in the PACU of − 2 or below will not be questioned regarding POD or pain.
The 3D-CAM is a reliable, validated diagnostic assessment tool for delirium, based on a structured 3-min interview to identify the presence of POD and was translated and validated for the use in German [40, 41]. Based on the principle of the CAM method, “(…) the algorithm is considered positive if following features are present: Feature 1) Acute onset or fluctuating course and Feature 2) Inattention and either Feature 3) Disorganized thinking or Feature 4) Altered level of consciousness.”
If a patient is identified as delirious based on the 3D-CAM, the RASS score will be used to determine the phenotype of the delirium at the timepoint of the visit: hypoactive (RASS − 5 to − 1) or hyperactive (RASS + 1 to + 4).
Furthermore, the 3D-CAM-S score will be calculated from the 3D-CAM assessment. The 3D-CAM-S is a validated method derived from the 3D-CAM diagnostic interview for assessing delirium severity, demonstrating excellent agreement with the commonly used delirium severity scale, CAM-S Short Form, and is designed to provide prognostic information, monitor delirium progression, and evaluate treatment response in older patients undergoing major elective non-cardiac surgery [42].
The Numeric Rating Scale (NRS) is a self-report measure of pain intensity on a scale of 0 (no pain) to 10 (worst possible pain), used for assessing a patient’s self-reported pain level.
Criteria for discontinuing or modifying allocated interventionsPatients may prematurely drop out of the study under the following conditions:
A premature end of the study or termination of the entire study may be considered under the following circumstances:
Strategies to improve adherence to interventionsThe study involves a single-session transcranial electrical stimulation (tES) intervention in the post-anesthesia care unit (PACU), administered and supervised by study staff immediately after surgery. This controlled setting minimizes the chances of non-adherence, as patients are continuously monitored. The brief duration of the intervention (20 min) allows seamless integration with standard PACU procedures, further reducing the risk of protocol deviations. Together, these factors ensure a high level of adherence without the need for additional compliance strategies.
Relevant concomitant care permitted or prohibited during the trialApart from the intervention and the close monitoring for POD during the postoperative visits, the participation in the study will not further affect the care of patients. Concerning the perioperative care, the anesthetic management protocols will not be modified by the trial. Induction and maintenance of anesthesia will be conducted according to the standard operating procedure of the clinic. The treating anesthesiologist will have access to the routinely used neuromonitoring devices and the indices of depth of anesthesia. If patients develop a POD, the treatment of productive delirious symptoms with antipsychotic drugs will be administered as prescribed by the treating ward physician.
At the Greifswald University Hospital, a delirium prevention unit has been implemented in the routine care of hospitalized patients of four departments (general surgery, orthopedy, internal medicine, and neurology). All patients over 65 years of age are screened daily by the unit, and non-pharmacological delirium prevention interventions are undertaken. Patients who are enrolled in the trial and admitted to one of these departments will not be visited or accompanied by the delirium prevention unit.
Provisions for post-trial careN/a. No provisions for ancillary and post-trial care are expected to be relevant to this study.
Outcomes Primary outcome measureIncidence of POD as defined by having at least one positive 3D-CAM within the 10 visits in the 5 postoperative in-hospital days.
Secondary outcome measuresDuration of POD (days between first positive 3D-CAM score and last positive 3D-CAM score)
Maximal POD severity (3D-CAM-S)
Median and interquartile range of POD severity (3D-CAM-S)
Delirium phenotype (RASS)
Adverse events
Incidence of emergency delirium in the PACU (PACU-D) as defined by having at least one positive 3D-CAM score in the PACU
Postoperative pain in the PACU (NRS)
Postoperative pain in the five first postoperative days (NRS)
Presence of postoperative nausea and vomiting (PONV)
EEG biomarkers from postoperative 64-channel EEG recordings including but not limited to total power, power within frequency bands, measures of periodic activity (power, center frequency, bandwidth), measures of aperiodic activity (offset, exponent), phase-lag-index, entropy measures, and burst-suppression-ratio
Postoperative blood biomarkers
Additional covariatesPreoperative pain, attitude towards pain, and affective disorders (PPI, HADS, STAI, PCS, BRI, PSQ, DN4)
Preoperative cognitive score (MoCA)
EEG biomarkers from pre- and intraoperative EEG recordings
Preoperative blood biomarkers
Intraoperative data related to anesthesia: anesthesia management, vital parameters, complications
Surgical data: type of surgery, duration of surgery, complications
Clinical treatment data: demographics, medical history, sensory impairments (vision aids, hearing aids), medication history, preoperative substance abuse, intensive care unit stay, perioperative transfusions, complications, number and type of lines (e.g., intravenous lines, central venous catheters, arterial blood pressure monitoring, nasogastric or percutaneous feeding tube, suprapubic or urinary catheter, possibly other drains), discharge/transfer destination, length of stay
Participant timelinePatients will receive one session of tES and will be visited postoperatively for 5 days (Table 1).
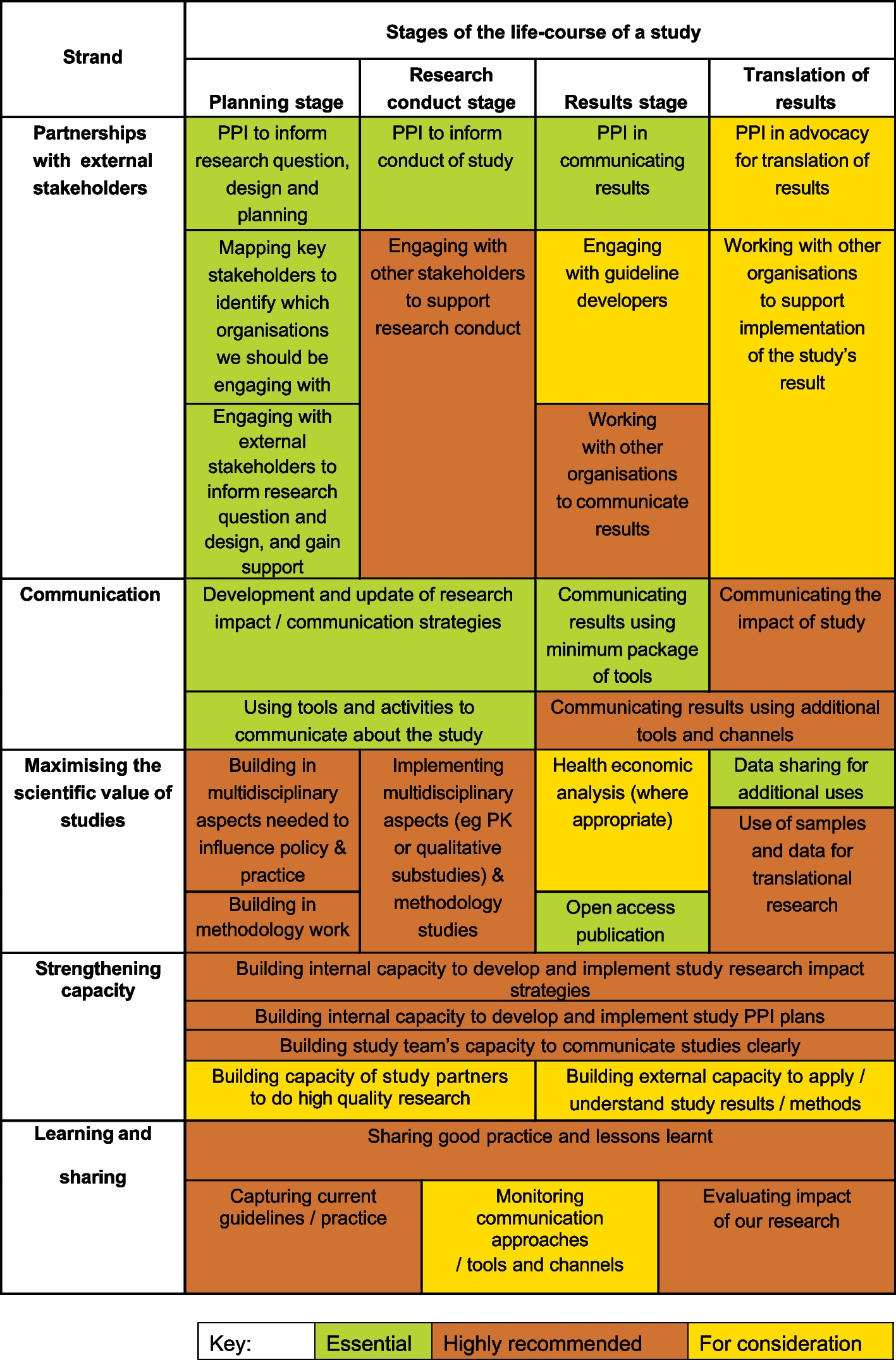
Table 1 Schedule of intervention and visitsSample sizeFor the effect of tDCS on the frequency of postoperative delirium, the trial by Tao and colleagues observed a reduction from 19.7 to 4.9% [35] (odds ratio: 4.761). A previous study on the incidence of POD among general surgical patients at Greifswald University Hospital showed a prevalence of 22.2% [42]. We assume an effect similar to those of Tao et al. To demonstrate such an effect between the tACS group and the sham-stimulation group using a chi-square test with a power of 80% and a one-sided significance level alpha of 0.05, a group size of N = 60 is required. With 3 groups, and an expected dropout rate of about 20%, in total N = 225 participants should be included (Fig. 3).
Fig. 3
Flow-chart of the study processes. tACS transcranial alternating current stimulation, tDCS transcranial direct current stimulation
RecruitmentTo achieve adequate participant enrolment, patients eligible for the trial will be screened daily by VB and SL and all patients meeting all the inclusion criteria and no exclusion criteria will be asked to participate in the trial. Due to the large number of operations conducted daily in the departments of interest at Greifswald University Hospital, we do not expect problems with the recruitment of patients.
留言 (0)