
記住我








All three interventions tested in the trial are in line with current treatment guidelines; however, the optimal treatment strategy for patients fulfilling the trial inclusion criteria has yet to be identified.
Intervention descriptionAll patients will be treated according to current national guidelines at the discretion of the treating physician. Long-term anticoagulation will be planned by the treating physician according to patient preferences. As a minimum, oxygen saturation, blood pressure, heart rate, and telemetry should be measured every hour for the first 24 h.
At the time of the diagnosis of intermediate-high risk PE, it is expected that most patients will be treated with unfractionated heparin (UFH) or Low molecular weight heparin (LMWH) according to site protocol. As per national guidelines, this adheres to the “wait-and-see” approach to this patient population in whom a risk of deterioration is present, which may require immediate full-dose thrombolysis or surgical embolectomy. To allow for such an up-scaling in treatment, anticoagulation with heparins is continued for at 24–48 h as per the discretion of the treating physician.
Inclusion in the trial will thus add treatment with low thrombolysis with or without USAT in two-third of the patient population.
Low-dose thrombolysis for IV infusionFor systemic thrombolysis, 20 mg of rtPA is dissolved in 20 ml of sterile water and further diluted into a total volume of 250 ml isotonic saline. The rtPA solution is infused in each catheter over 6 h (infusion rate approx. 41 ml/h) in a separate IV line.
Low-dose thrombolysis as part of USATPatients allocated to low-dose thrombolysis via USAT are transferred to Rigshospitalet as soon as possible, in order to initiate treatment with USAT within 12 h post-randomization. Two USAT catheters are placed in the lower pulmonary artery under fluoroscopic guidance via access from the femoral vein. Vein puncture is performed under ultrasound guidance, and 2 6 Fr. sheaths are placed using the Seldinger technique.
Immediately after placing the catheter, the ultrasound-emitting crystal catheter is placed in the USAT catheter, and an infusion of 10 mg rtPA (20 mg vial, separated into 2 × 250 ml isotonic saline solution) is administered over 6 h (infusion rate 41 ml/h). Further 30 ml/h of isotonic saline infusion as a coolant is infused via the catheters.
As most patients are expected to have bilateral clots, two USAT catheters are placed. If only unilateral PE is found, the 20 mg of rtPA is infused in the catheter instead of the 10 mg for bilateral catheters.
After 6 h the infusion of rtPA is terminated, and the USAT catheters are removed, leaving the sheaths in place. After an additional 2 h, the sheaths are removed under manual compression of the puncture site for 10 min. One hour after removal of the sheaths the patient is confined to bed with a maximum of 30 degree elevation of head rest. Analgesics and sedatives (benzodiazepines) may be ordered for patients’ comfort.
Patients are transferred to Rigshospitalet after initiation of heparin. If LMWH administration is less than 6 h away, no bolus UFH dose is given. Otherwise, a bolus dose of 60 IE/kg (max. 4000 IE) is given, followed by an infusion of 12 IE/kg/h (max. 1000 IE/h as initial infusion rate). The UFH is administered in a separate IV line. Infusion rates are adjusted according to Activated partial thromboplastin clotting time (APTT), targeting 1.5–2.5 times longer APTT than the baseline value. APTT is measured every 4 h for the first 8 h, and then longer time intervals can be ordered. Activated Clot Time (ACT) of 160–180 s can be used as an alternative.
The patients transferred to Rigshospitalet were admitted here until the 48–96-h CTPA was performed and then transferred back to the local hospitals. All other participating sites were level 2 with specialized cardiologists attending.
Criteria for discontinuing or modifying allocated interventionsIf local reaction or bleeding occurs when treated with rtPA IV or via USAT, the infusion is paused, and the attending physician will decide whether to terminate the infusion or not. The T1/2 of rtPA is 5 min.
If a patient clinically deteriorates despite relevant treatment, whether it is heparin or heparin and low-dose thrombolysis IV/USAT, upscaling treatment to full-dose thrombolysis (rtPA 100 mg IV over 2 h) will be initiated in accordance with current guidelines.
Strategies to improve adherence to interventionsAll physicians and nursing staff involved in the care of the study patients are trained on a regular basis in the allocated treatment strategies and obtainment of relevant endpoints. The steering group is available for advice if needed by the treating physician.
Relevant concomitant care permitted or prohibited during the trialThe study intervention ends after completion of follow-up CTPA conducted 48–96 h post-randomization. Concomitant care adheres to established clinical standard protocols including transition to oral anticoagulant treatment.
Provisions for post-trial careUpon hospital discharge, patients are invited for a 3-month follow-up at Rigshospitalet. The follow-up includes CTPA, transthoracic echocardiography, blood sampling, 6MWT, and questionnaires.
Outcomes Co-primary endpointReduction in refined Miller score (RMS) at 48–96 h post-randomization (score of thrombus involvement and segmental flow) [13, 14] comparing thrombolysis groups (combining groups with and without USAT) to UFH/LMWH group, p < 0.01 (two-sided), full study population, n = 140 vs. n = 70.
Reduction in RMS at 48–96 h post-randomization comparing thrombolysis administered via USAT or IV, p < 0.04 (two-sided), population treated by low-dose thrombolysis, n = 70 vs n = 70.
Secondary endpointsBleeding complications (major and minor bleeding complications according to the thrombolysis in myocardial infarction classification)
Duration of index admission, including hospital-based rehabilitation
Dyspnoea index (visual analog scale) after 48–96 h and after 3 months
FiO2, blood pressure, and respiratory rate, heart rate at the time of follow-up CTPA
Mortality in the three groups (log-rank), and hazard ratio in multivariable analysis using the UFH/LMWH as a reference.
Incidence of TR gradient > 40 mmHg at 3 months follow-up echocardiography
6MWT at 3 months follow up comparing the three groups.
Quality of life at 3 months follow-up comparing the three groups (PEmb-Qol and 5Q-5D-5L)
We were unable to systematically collect data for the following pre-planned endpoints: reduction in D-dimer from baseline to 48–96 h post-randomization, Relative reduction in TnI/T from baseline to 48–96 h post-intervention, and reduction in NT-pro-BNP at 48–96 h and 3 months. These secondary endpoints will not be reported in the primary publication.
We were unable to systematically collect data for the following pre-planned endpoints: reduction in D-dimer from baseline to 48–96 h post-randomization, Relative reduction in TnI/T from baseline to 48–96 h post-intervention, and reduction in NT-pro-BNP at 48–96 h and 3 months. These secondary endpoints will not be reported in the primary publication.
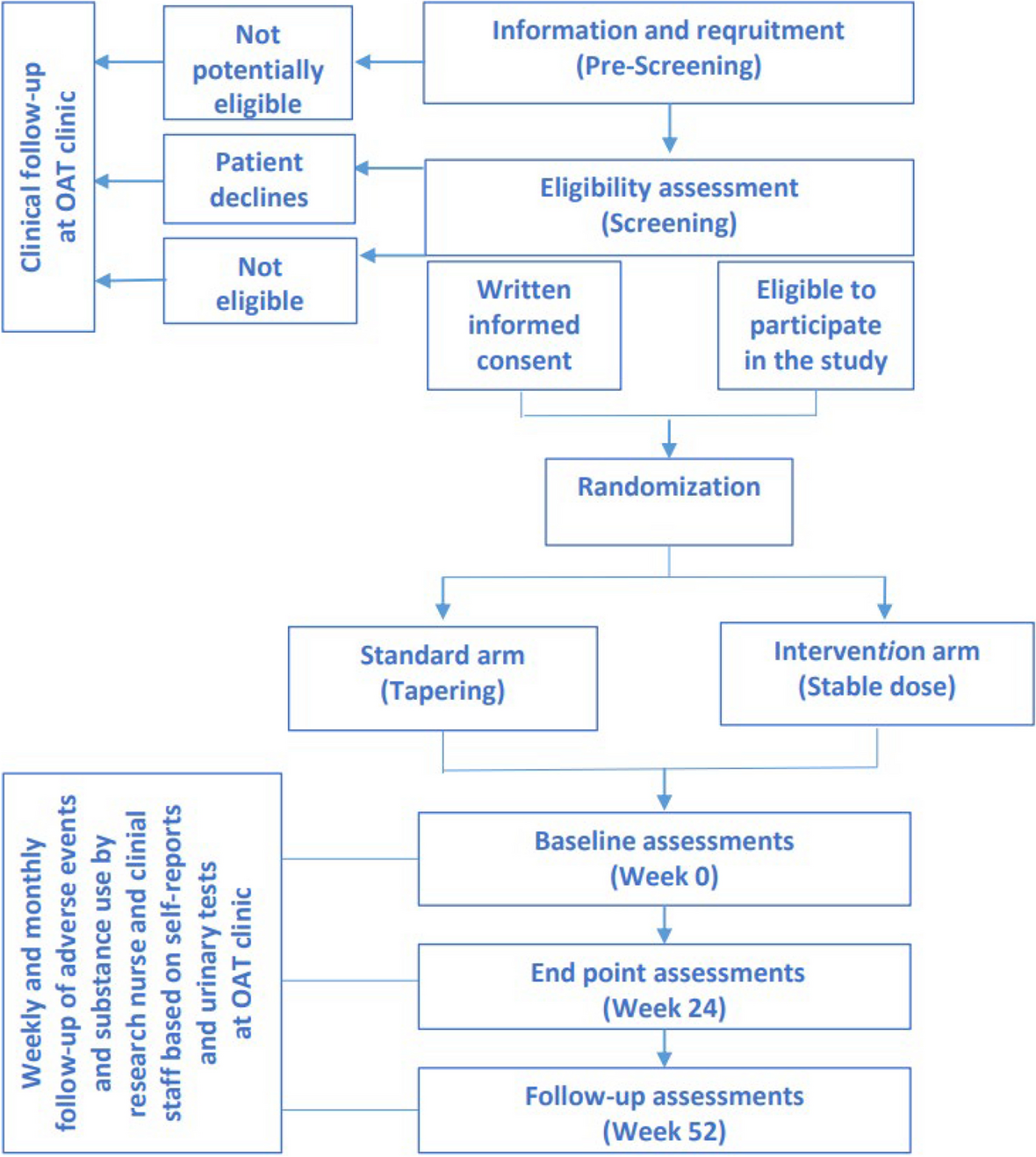
Participant timelineThe flowchart is shown in Fig. 1.
Fig. 1
Flowchart of patient enrolment and participation. CT, computed tomography; UFH, unfractionated heparin; LMWH, low molecular weight heparin; USAT, ultrasound-assisted thrombolysis; NOAC, novel oral anticoagulation; VKA, vitamin K antagonist; h, hour; m, month; y, year
Sample sizeThe power of the trial is calculated as two co-primary endpoints, sharing a combined α-level of 0.05.
A mean RMS of 18 ± 7 is expected at baseline [14]. A variance component model (proc mixed, SAS enterprise ver. 8,4, Cary, NC) was applied.
The treatment effect is expected to be a reduction in RMS of 2 points (11%) in the UFH/LMWH group after 48–96 h (extrapolation from [13]), whereas the reduction in RMS in both thrombolysis groups is expected to be 6 points (33%) [13]. The net effect of thrombolysis by USAT is expected to be similarly efficacious.
The first co-primary endpoint evaluates the effect of the intervention of thrombolysis comparing RMS in the UFH/LMWH group to RMS in the combined groups of low-dose thrombolysis with or without USAT (1:2).
Planning inclusion of 165 (3*55) patients will give a power of 0.8 whereas 210 (3*70) patients will give a power of 0.90, with an α of 0.01 for the primary endpoint.
The second co-primary endpoint evaluates the effect of low-dose thrombolysis administered by USAT or IV will yield a power of 0.9 by the inclusion of 140 patients (1:1) with an α-level of 0.04, assuming a 22% reduction or greater reduction in RMS in the USAT group compared the IV group.
The trial is planning to include 210 patients, with 70 patients assigned to UFH/LMWH, 70 to low-dose thrombolysis without USAT, and 70 assigned to low-dose thrombolysis with USAT initiated within a mean of 12 h from randomization.
RecruitmentEach inclusion site is routinely visited by a member of the steering group who provides updates and trains new staff members on patient screening procedures and study protocol, thereby ensuring consistent patient enrollment.
留言 (0)