
記住我





The comparator is tapering with diazepam or oxazepam in maximum 20 weeks according to the applied clinical procedure in OAT clinics which is based on the Norwegian OAT guidelines recommending gradual tapering and discontinuation of benzodiazepines as the standard treatment of benzodiazepine dependence.
Intervention descriptionParticipants in the intervention arm will receive stabilizing agonist treatment with 15–30 mg/day diazepam or equivalent dosages of 50–100 mg/day oxazepam in 26 weeks. Participants in the standard arm will receive tapering with diazepam or oxazepam in maximum 20 weeks according to the applied clinical procedure in OAT clinics. The type of benzodiazepine prescribed (diazepam or oxazepam), the start dosages, and the duration of tapering will be based on the degree of dependence, the dosages of illicit benzodiazepines used prior to study entrance, and the individual’s clinical condition [22]. Accordingly, a customized tapering plan will be suggested to each participant within the framework of the study procedures.
For both arms, treatment initiation and follow-up will be conducted at OAT outpatient clinic where they already receive OAT and relevant care including voluntary psychosocial interventions. The study medications will be prescribed by the physicians in the OAT clinics in accordance with the protocol and will be delivered either at the OAT clinic or at a pharmacy in line with the applied standards for OAT follow-up. Commercial tablets and standard medication labels will be used, tagged with trial log numbers. All the costs related to the medications, preparations, and observed intakes will be covered by the OAT clinics (through public assigned funds). The medications will be used in line with national guidelines, and the project will strive to comply with the Good Clinical Practice (GCP) [10, 23].
Criteria for discontinuing or modifying allocated interventionsThe stop criteria for the individual participant are defined at least based on non-compliance, unexpected adverse events, or other safety considerations such as use of large amounts of highly potent street benzodiazepines with clinically observed signs of overdosing. In addition, medication can be withheld in the case of deviation from urinary test procedures that can affect measuring the trial primary outcome. Participants who have discontinued protocol-based treatment will be motivated to continue to participate in all remaining research interviews and assessments. For those participants who revoke their consent for the entire study, no further data will be collected from the participant.
Strategies to improve adherence to interventionsMedication choice between oxazepam and diazepam will be individualized based on patient preferences, medical history, and present health condition. The prescription method will also be assessed individually and based on the patient’s treatment course (i.e., prescribed by the clinic physician and ordered through the related clinic or pharmacy). All participants will be encouraged to initiate the treatment according to the protocol, with data collected on prescription pickup and treatment initiation dates. In addition, for those receiving medications in the clinics, frequencies, and observation of doses taken will be noted. Self-reported data on medication adherence and compliance will be obtained for all participants. Medication adherence and compliance will be assessed through a combination of prescription pickup frequency, self-reported adherence, observed intake, and urinary tests.
Related authorized clinical study-monitoring organs in each health county will visit the study sites on a regular basis to ensure the following requirements: informed consent process, reporting of adverse events and all other safety data, adherence to protocol, maintenance of required regulatory documents, facilities, and data completion on the case report files (CRFs) including source data verification. Additionally, a data monitoring committee (DMC) comprising two independent professionals (a clinician and a researcher) and a statistician will ensure the safety and wellbeing of trial patients and will assist and advice the coordinating and principal investigators to protect the validity and credibility of the trial.
Relevant concomitant care permitted or prohibited during the trialAll the participants will receive OAT and the related care as usual. Study medications will mainly be administered under supervision by the OAT clinic or pharmacy staff. Individually assessed, the participants will receive some of the doses as take-home-dosages for self-administration. Assessments of observed intake frequency and “take-home doses” will follow the same agreement that applies to OAT medications, and any changes will be assessed by the prescribing OAT physician after discussion in interdisciplinary team. Project managers will be informed of any changes. In any case, all participants should attend the OAT outpatient clinic daily or at least once weekly for clinical observations. Every participant should, regardless of the delivery agreement, have frequently clinical observations and assessments for the first 2 weeks after starting prescription (in both study arms) to ensure treatment safety. After this period, they follow the delivery agreement as before.
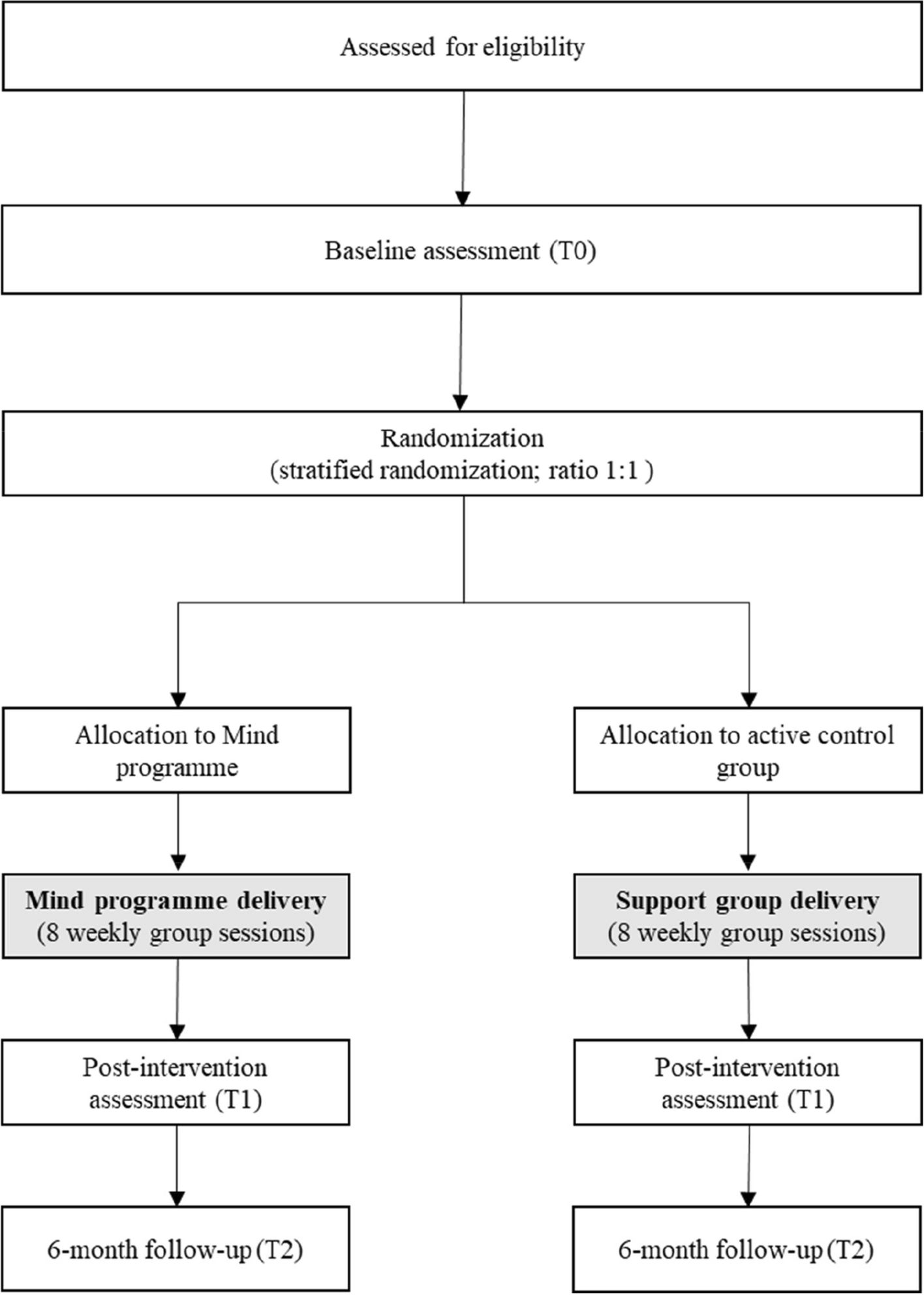
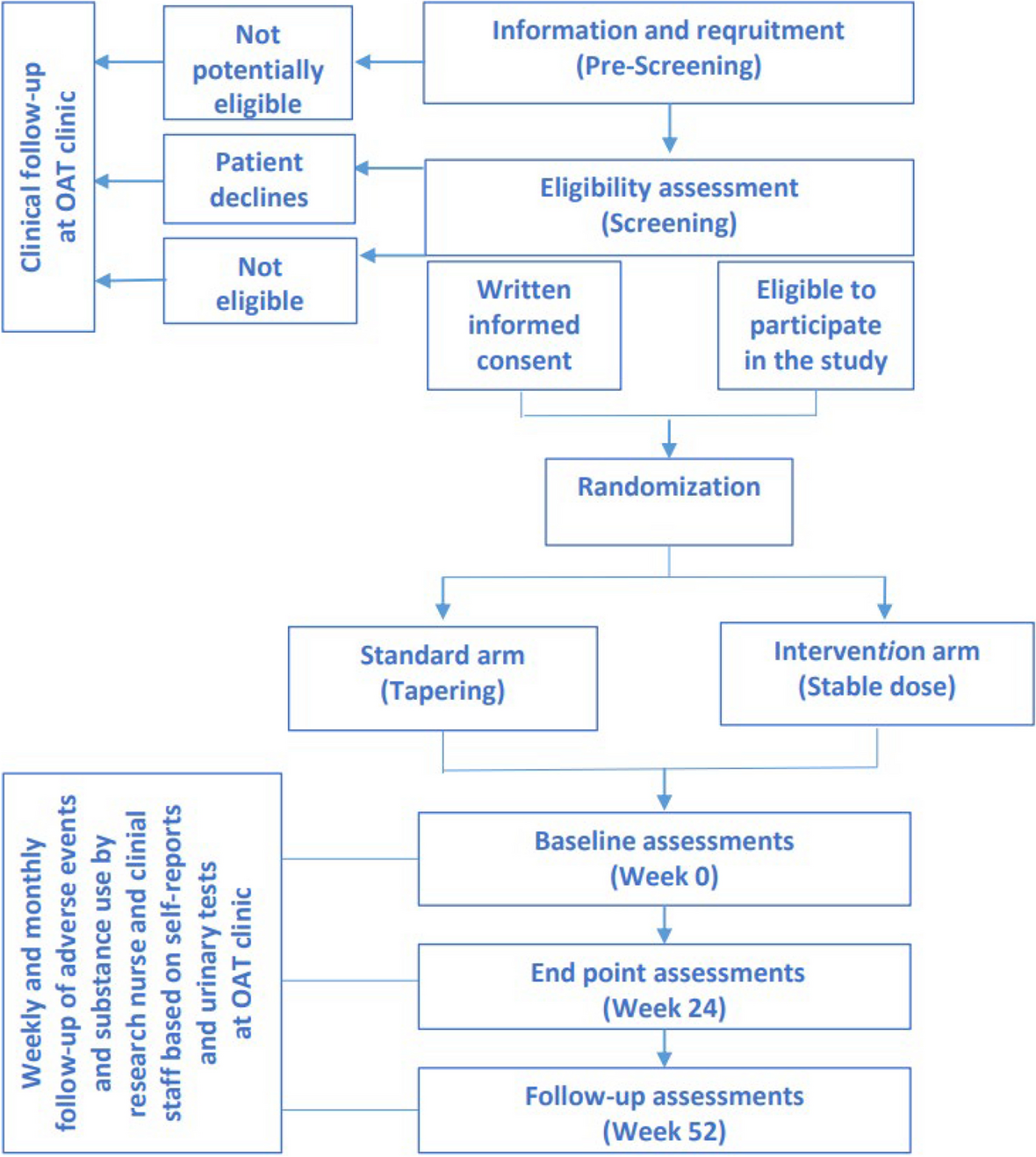
Clinical and biological follow-up of participants and systematic report of potential adverse effects will be organized according to international GCP guidelines. The participants will be assigned to the scheduled assessments by research nurses and/or clinic physicians in line with the study protocol. The assessments will be performed at baseline, and at week 24 in addition to a follow-up assessment at week 52 after entering the trial. The OAT staff or research nurses will follow up the participants weekly at OAT clinics or by home-based visits if needed, with consultations including self-reports on illicit use of benzodiazepines and other substances, adverse events as well as monthly randomized urine drug screening tests during the trial period (Fig. 1 and Table 1).
Fig. 1
Flow-chart of the study procedures. Legend: Potential participants will be screened for eligibility. Individuals, who meet the eligibility criteria and provide written informed consent to participate, will be randomized either to a stabilizing dose with diazepam or oxazepam, or tapering using the same medications. The primary endpoint is at week 24 with a follow-up visit at week 52. OAT: opioid agonist treatment
Table 1 Schedule of activities during the study periodProvisions for post-trial careAt the end of trial period, each participant will be individually assessed to receive further clinical follow-up as indicated. Participants who receive stabilizing treatment with prescription benzodiazepines during the 26-week study period will undergo individual clinical assessments upon trial completion. Some participants may continue with stabilizing treatment, while others will have their prescriptions stepped down and discontinued following current guidelines. Participants in the standard treatment arm will receive ongoing treatment and follow-up using conventional approaches after tapering of medications.
Participants will be informed about these individual assessments at the study enterance. Clinical observations throughout the study period will provide insights into outcomes for participants in each study arm. Decision-making following the project’s conclusion will be based on these outcomes, aligning with the conditions governing benzodiazepine continuation outlined in the study protocol. Assessments will occur both upon completion of the intervention (after week 26) and at the end of the project period (after week 52).
OutcomesPrimary outcome measure is:
Secondary outcome measures collected at baseline and week 24 will include:
Mental health symptoms score using Hopkins symptom checklist (SCL-10) [24]
Health-related quality of life score using 5-dimensional, 5-level Euro Quality of life questionnaire (EQ-5D-5L) [25]
Reaction time for cognitive performance using a simple reaction time test [26]
Risk of violence behavior using Brøset violence checklist (BVC) [27]
Satisfaction with the treatment using visual analog scale (VAS) from 0 to 10
Retention rate in OAT (number of drop-out days during the trial period)
Self-reported frequency of use of alcohol and illicit substances including benzodiazepines, and urine drug screening for alcohol and illicit substances other than benzodiazepines
Number of non-fatal overdoses and death (if any)
Cost-effectiveness of intervention
Participant timelineThe time schedule of enrolment, interventions, assessments, and visits for participants is shown in Table 1.
Sample sizeThe sample size calculation is based on clinical experiences due to no existing empiric assumption. The prevalence of use of illicit benzodiazepines during standard treatment is assumed to vary from 50% to 80%. We have used an “illegal” index which is defined as the proportion of positive urinary tests confirming the use of illicit benzodiazepines and is considered continuous. We set the minimal clinically relevant difference between the groups—regarding the illegal index at week 24—to 0.3, and the required power to 0.8 at two-sided significance level of 0.05. There is no valid data to estimate the standard deviation. Assuming a risk of 0.5 to 0.8 for the use of illicit benzodiazepines in the standard treatment group (p1), and an expected difference of 0.3 between the two arms (p1-p2), we need 43 patients per group (Fig. 2). Assuming a drop-out rate of 20% we need 54 patients in each group, 108 in total, to achieve sufficient power [28].
Fig. 2 Recruitment
Recruitment Enrollment was commenced autumn 2022 and will continue until the required number of eligible participants is enrolled in the trial. For both arms, all the clinical stages of the study—including recruitment, information, obtaining written consent, clinical interviews, and completing the study surveys using appropriate instruments, and treatments—will be performed by research nurses and/or physicians to ensure independence. Six OAT sites are involved in the trial conduction to obtain the required sample size.
留言 (0)