Our retrospective cohort study found that the elevated baseline RFM was associated with an increased risk of fatal, nonfatal CVD events, and all-cause mortality in NGT, prediabetes, and diabetes, and these associations were modified by glucose tolerance statuses. We identified mediating and synergistic effects in the associations between RFM and outcomes, and through joint analysis, we pinpointed the subclassification with the highest HR among 12 groups. These findings could influence clinicians' assessment of high-risk cases and lead to more personalized prevention strategies. In addition, RCS analyses indicated the dose–response relationships between RFM and the outcomes and identified the potential RFM cutoffs. Finally, among all obesity indices including RFM, BMI, WC, and WHR, RFM displayed the largest predictive performance in all glucose tolerance statuses.
Our study reiterates the associations between RFM and the risk of CVD events and all-cause mortality, which is consistent with previous studies [4, 5, 8, 26,27,28]. The present study corroborated these associations and extended these in the Asian population with cohort epidemiological evidence. Mechanically, excessive body fat (increased RFM levels) causes adipocyte dysfunction by aberrant release of pro-inflammatory and adipocytokines, which may be involved in vascular dysfunction and systemic insulin resistance, subsequently triggering CVD and death [2,3,4,5,6, 8]. However, previous studies only focused on the general population. The evidence on populations with NGT, prediabetes, and diabetes, respectively is scarce [2, 4,5,6, 8]. The present study revealed that the associations between RFM and outcomes were significant in all glucose tolerance statuses, respectively. In line with our result, Asgari et al. reported that general obesity defined as BMI ≥ 30 kg/m2 increased the risk of CVD mortality and all-cause mortality events in all glucose tolerance statuses, respectively, from three longitudinal Iran studies [29]. However, Asgari et al. reported that the association considering the outcomes of CVD was non-significant [29]. We assume this is because the reason that Asians exhibit several morphological characteristics and have a shorter height, greater percentage of body fat, and substantially bigger trunk adiposity and waist circumference compared with Caucasians of the same age and BMI, which are risk factors for CVD and death [30].
Furthermore, the modified effects including mediating and interactive roles of glucose tolerance status in the associations between RFM and fatal, nonfatal CVD events, and all-cause mortality have been less addressed. The present study therefore delved into the mediation analysis, interaction analysis, and joint analysis. Firstly, mediation analysis found that glucose tolerance status partially mediated the associations between RFM and risk of CVD and all-cause mortality. Consistently, Suthahar et al. found RFM is strongly associated with new-onset diabetes from a prospective cohort study in the Netherlands [3]. Lu et al. reported that BMI was linked to diabetes in a cohort study including 20,944 participants in the NAGALA [31]. Mechanically, obesity (high levels of RFM) causes adipose tissue fibrosis by increased rates of fibrogenesis, strengthens inflammation by increased proinflammatory macrophage and T cell content, and the production of exosomes, leading to both insulin resistance and β-cell dysfunction, and finally results in prediabetes and diabetes [32,33,34,35]. Furthermore, prediabetes and diabetes could induce CVD and death via abnormalities in cardiac metabolism, physiological and pathophysiological signaling, and the mitochondrial compartment, in addition to oxidative stress, inflammation, myocardial cell death pathways, and neurohumoral mechanisms [21]. Healthcare practitioners should assess glucose tolerance status in persons with high RFM, leading to more personalized, effective prevention strategies.
Secondly, interaction analysis revealed significant multiplicative interactive effects between RFM and glucose tolerance status on fatal, nonfatal CVD events, and all-cause mortality, which indicated that RFM and prediabetes and diabetes could induce CVD and death in a synergistic method. In line with our study, Shen et al. also found the synergistic effects of obesity and high hemoglobin A1c status on increased levels of high-sensitivity C-reactive protein in a cross-sectional Chinese study that included 1,630 adults aged 18–75 years [36]. Xu et al. found the interactive effect of diabetes with BMI for survival among 4,515 recipients of liver transplants [37]. The multiplicative interactive effect means that the combined effect is larger than the product of the individual effects of RFM and prediabetes and diabetes. We assumed this synergistic effect may be due to a positive feedback mechanism between RFM and prediabetes and diabetes. On the one hand, obesity leads to prediabetes and diabetes by both insulin resistance and β-cell dysfunction via pathways about fibrogenesis and inflammation [32]. On the other hand, prediabetes and diabetes cause obesity by: (i). improper metabolism of glucose in cells, leading to an excessive generation of reactive oxygen species, which harm cellular function and insulin receptors, causing insulin resistance and therefore adipose tissue accumulation [32, 36, 37]. (ii). hyperglycemia is often accompanied by an elevation of free fatty acids [32, 36, 37]. Hence, the reciprocal promotion of high RFM and hyperglycemia contributes to the development of metabolic and inflammation disorders, exacerbating the progression of CVD and mortality [32, 36, 37]. The interactive effects underscore the importance of considering RFM and glucose tolerance status jointly in CVD and death risk assessment.
Thirdly, with the combination of mediating and interactive effects, we conducted the joint association and identified the subclassification that displayed the highest HR among the 12 subclassifications. When comparing persons with NGT and RFM in the first quartile, the greatest HRs were observed in individuals with diabetes and RFM in the fourth quartile among 12 distinct groups for both fatal and nonfatal CVD events. Asgari et al. reported that individuals with diabetes and obesity exhibited the highest HR compared with other diabesity phenotypes for risk of CVD, CVD mortality, and all-cause mortality in an Iran cohort study [29]. Whereas, we observed that those who have diabetes and a high RFM in the third quartile for all-cause mortality had the greatest HR, which was slightly higher than those with diabetes and a high RFM lying in the fourth quartile based on NGT&RFM Q1 as reference. The difference may be due to the following reasons. First, there may be a potential nonlinearity in the joint effect of RFM and prediabetes and diabetes for all-cause mortality. Second, Asgari's research classified obesity as a BMI of 30 kg/m2 or above, while we categorized participants based on quartiles of RFM. Third, the ethnic differences may also account for the disparity [30]. Join analysis could significantly influence how clinicians assess high-risk individuals, lead to more personalized and effective strategies, and underscore the importance of comprehensive prevention strategies that combine obesity with hyperglycemia.
By subgroup analysis, we observed that RFM and fatal CVD events and all-cause mortality showed more prominent relationships in the subgroup of females in all and those with diabetes. Differently, Zwartkruis et al., found that RFM was more greatly associated with CVD in males [5]. Most of the women included in our study were postmenopausal with a median age of 60.12 years old, while the median age was 45 years old in Zwartkruis’s study. With the absence of the protective effect of estrogen on CVD and death [38], females therefore exhibit a higher risk than men. Moreover, those with prediabetes displayed stronger HR in the subgroup of age < 60. This may be due to that in the subgroup of ≥ 60, the independent risk of RFM may be attenuated by other stronger risk factors. Furthermore, RCS suggested dose-dependent associations between RFM and outcomes and identified the relative cutoffs for clinical practice. Wang et al. also found a U-shaped RCS in males and an approximately J-shaped RCS in females [4]. The RCS were mostly approximately J-shaped in our cohort, which may be because most subjects were females. In addition, by comparison with other obesity indices including BMI, WC, and WHR, RFM exhibited the highest predictive performance. Shen et al. also found the RFM had the highest AUC compared with other indices in a cross-sectional study consisting of 11,532 adult Chinses participants [8]. We extended this with cohort epidemiological evidence for Asians.
The strengths of this study are as follows. First, the present study is the first to investigate the associations between RFM and CVD events and all-cause mortality in NGT, prediabetes, and diabetes, respectively, and investigate the modified effect including mediating and interactive effects of glucose tolerance statuses on these relationships, which provides practical implications for clinical practice of risk stratification and comprehensive prevention. We also conducted the joint analysis and identified the subclassification that exhibited the highest HR among 12 subclassifications, which might have a substantial impact on how medical practitioners evaluate high-risk cases and could result in the development of more personalized, effective prevention strategies. Second, we filled the knowledge gap of the association between RFM and the risk of CVD events and all-cause mortality with the cohort epidemiological evidence for the Asian population, which has been rarely reported. Third, the present study discovered the dose-dependent association between RFM and outcomes and provided potential RFM cutoffs by RCS analyses, which lack evidence in population-based cohorts for Asians. Fourth, we compared the predictive performance of RFM with other standardized obesity indices including BMI, WC, and WHR, and extended the comparisons to different glucose tolerance statuses. Fifth, the present study was performed in a large, longitudinal, contemporary, population-based cohort with a follow-up of up to 5 years.
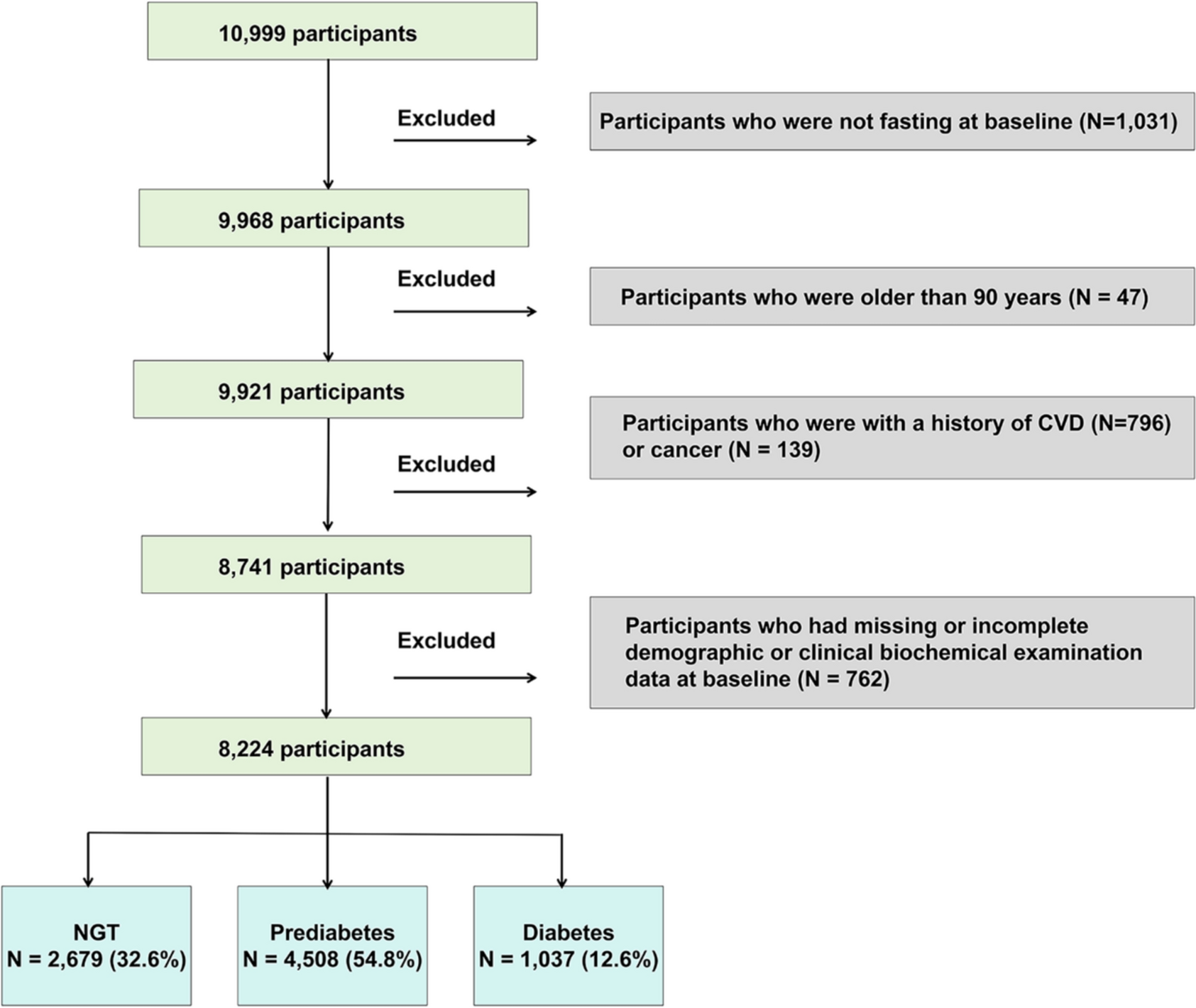
This study has several limitations. First, while RFM accurately predicts fat mass, it cannot distinguish between visceral and subcutaneous fat. Imaging techniques like magnetic resonance imaging can provide more precise fat compartment measurements but are not feasible for large cohorts. However, RFM is easy to calculate, gender-specific, non-invasive, cost-effective, and more accurate in estimating total body fat [5, 7]. Second, the relatively short follow-up duration reduced the number of clinical outcome events and affected the statistical power, but our findings were nonetheless meaningful. Hence, further investigations need to include more extensive sample sizes and extended follow-up durations. Third, although we adjusted for numerous potential confounders, other unknown or unmeasured variables, including diet, etc., may have influenced these associations. Fourth, it is important to note that this study only focused on people of Chinese ethnicity who were 40 years old or older. Therefore, further research is needed in other countries and across different age groups to confirm these findings. Fifth, the baseline analysis included 32.6% with NGT, 54.8% with prediabetes, and 12.6% with diabetes. Wang et al. [39] reported a prediabetes prevalence of 38.1% and a diabetes prevalence of 12.4% in a nationally representative Chinese sample of 173,642 adults. While our study's diabetes prevalence aligns with Wang's, the prediabetes prevalence was higher, likely due to the older average age in our cohort (60.1 vs. 51.3 years) [39]. Although our sample may not fully represent the general population, the study remains valuable as we analyzed each group (NGT, prediabetes, and diabetes) separately, making the results relevant to each group.

留言 (0)