
記住我
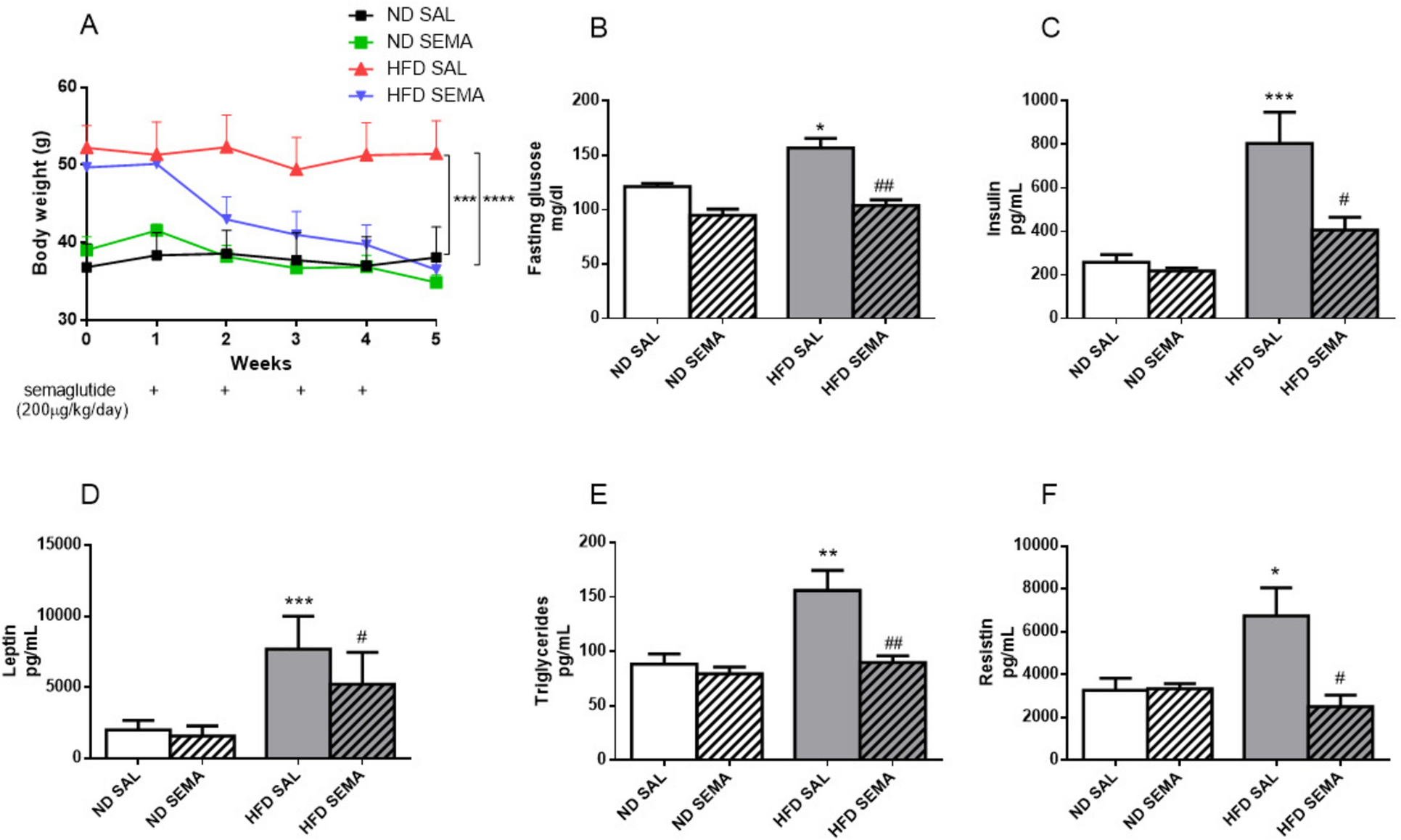
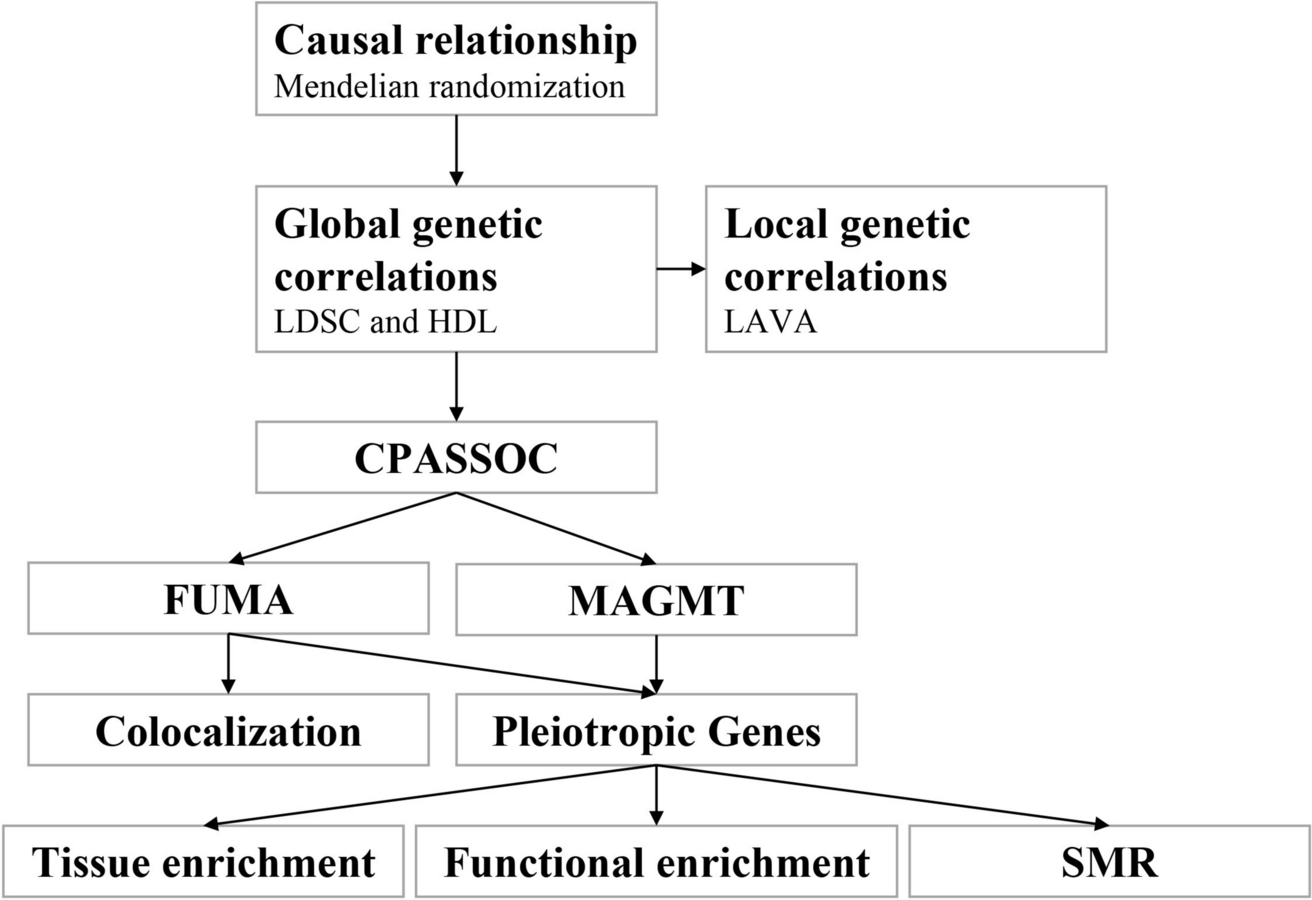
Recent studies have suggested that disorders in BMI and lipid metabolism associated with obesity may play an important role in the pathogenesis of diabetes [18,19,20]. As Lu et al. [18] demonstrated in their study based on NAGALA, significant correlations were found between BMI and diabetes risk for most lipid parameters, except for TC, LDL-C F, LDL-C S, and non-HDL-C. Similarly, a 3-year cohort study by Li et al. [19] indicated that residual cholesterol, rather than other traditional lipids or lipid ratios, was independently and positively associated with the future risk of diabetes in the general Chinese population. In contrast, Chen et al. [20] found that TG/HDL-C was positively correlated with diabetes risk, and the relationship between TG/HDL-C and diabetes incidence was nonlinear; when TG/HDL-C was less than 1.186, there was a strong positive association with diabetes incidence. Although these studies do not reach a unanimous conclusion, they all suggest that lipids may be an important mediator in the relationship between BMI and diabetes risk. Therefore, the current study aimed to further clarify the impact of a range of lipid parameters on the association between BMI and diabetes risk, which could provide important insights into the underlying pathogenesis and daily risk management of diabetes. The process of our MR analysis in the study is shown in Fig. 8.
Fig. 8
The process of MR analysis in this study
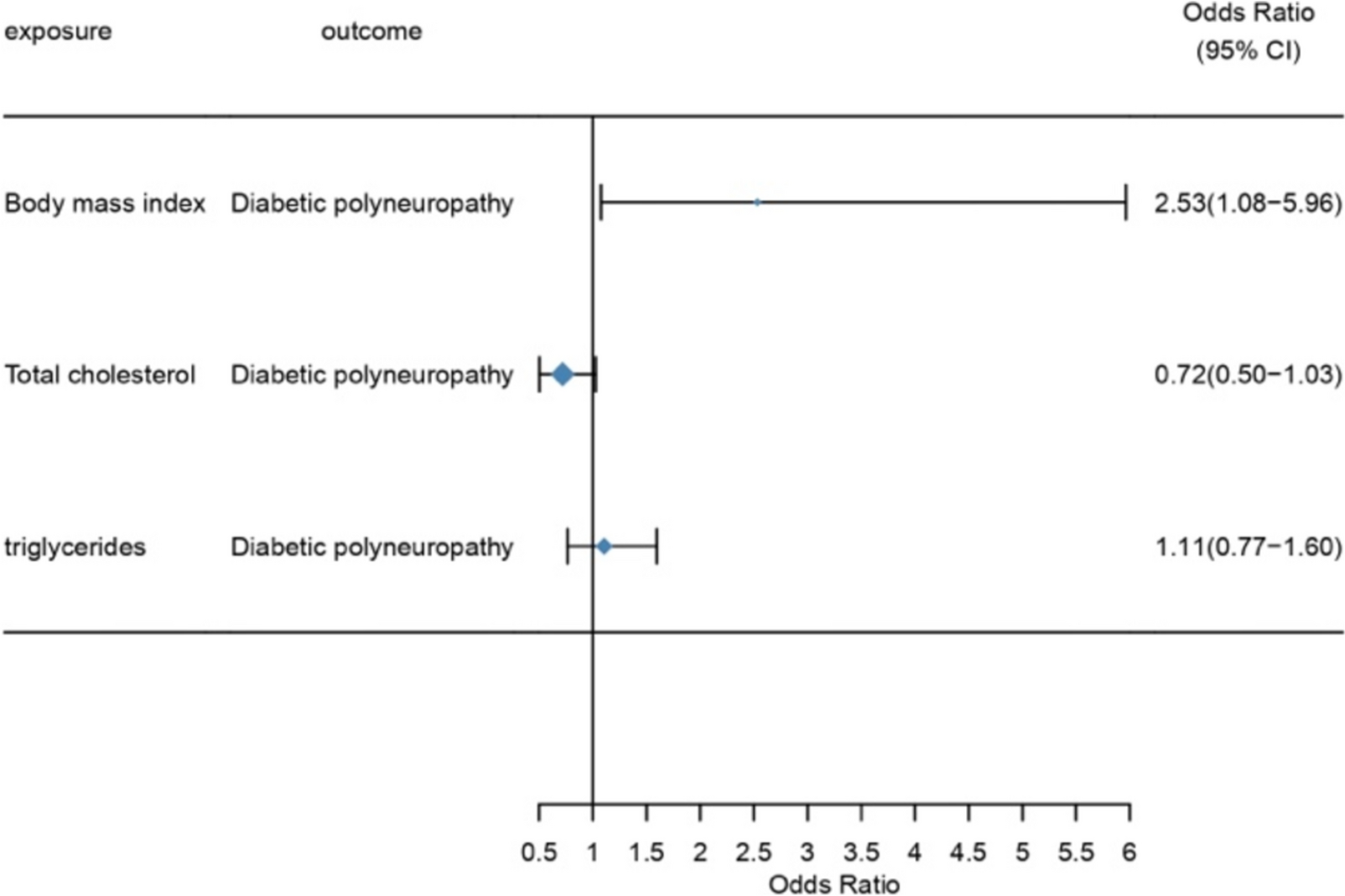
While our study demonstrates a significant association between BMI and DN risk, this finding contrasts with some previous studies that reported either no association or an inverse relationship between BMI and diabetic neuropathy [21]. While Valensi et al. [22] identified an inverse relationship between BMI and cardiac autonomic neuropathy. Tentolouris et al. [23] observed no significant differences in autonomic neuropathy prevalence between normal-weight and type 2 diabetes mellitus patients. These discrepancies may be attributed to differences in study populations, including variations in diabetes type, ethnicity, and disease duration. Additionally, our study employed MR to infer causality, minimizing confounding and reverse causation, whereas the studies primarily relied on observational designs. Such differences in statistical approaches may also explain the inconsistencies. Further research, including harmonized study designs and larger, more diverse cohorts, is needed to reconcile these conflicting findings.
Despite these differing findings, our study indicates a positive correlation between BMI and the risk of DN development, whereas no significant association was observed between total cholesterol (TC) or triglycerides (TG) and the risk of DN. These results suggest that BMI may be an independent risk factor for the progression of diabetic nephropathy, while the impact of lipid parameters may not be as pronounced as previously expected. This underscores the need for larger and more diverse studies to further elucidate the role of BMI in diabetes-related complications.
Obesity-induced neuropathic pain may be associated with the loss of small nerve fibers (SF) and oxidative stress [25]. The loss of SF can increase the risk of neuropathic pain, and as nerve loss or damage progresses, pain may be alleviated following nerve regeneration [26]. Inflammatory mediators play a critical role in distinguishing between painful and painless neuropathy, with elevated serum levels of IL-2 and TNF-α and reduced levels of IL-10 being key markers [27]. Additionally, 1-deoxysphingolipids and 25-hydroxyvitamin D have also been linked to obesity and neuropathic pain [28, 29]. In patients with obesity and hypertriglyceridemia, the high expression of inflammatory mediators may lead to oxidative stress, thereby causing neuropathic pain. Previous studies using Spearman correlation analysis have shown a significant relationship between 24-h urinary albumin excretion, triglycerides (TG), and BMI, suggesting that BMI and TG may exacerbate pain in patients with diabetic peripheral neuropathy (DPN) [30]. Logistic regression analysis further identified BMI, TG, duration of diabetes mellitus (DM), and 24-h urinary albumin excretion (24hUAlb) as factors influencing painful DN [31]. Obesity is also known to impair renal structure and function, making it a risk factor for chronic kidney disease [30]. However, our analysis did not observe a clear relationship between lipid metabolism and the risk of diabetic neuropathy, suggesting that further research is needed to establish this connection. Lipid metabolism is a complex process, and different lipid parameters may play varying roles under different pathological conditions [18,19,20]. Moreover, triglyceride and total cholesterol levels can be influenced by various factors, including diet, medications, and genetics. Thus, differences in study outcomes may be due to the inherent complexity of lipid metabolism [32].
Triglycerides (TG) are closely associated with the occurrence and progression of diabetic neuropathy (DN) [33] and are an independent risk factor for lower limb amputation in diabetic patients [34]. In individuals with diabetes, elevated TG levels, hyperglycemic toxicity, and reduced perfusion due to microvascular damage may form a distinct neurotoxic triad [35]. Although the specific mechanisms by which elevated TG induces DN are not fully understood, some studies suggest that disruptions in lipid metabolism within sensory and motor neurons may lead to neural cell damage and impaired nerve conduction [33].
However, our analysis did not find a potential relationship between TG levels and risk factors for DN, which contrasts with previous research findings. Additionally, our study did not observe a clear relationship between total cholesterol (TC) and the risk of DN. The relationship between BMI and DN, as well as the roles of TG and TC, may be modulated by other factors such as gut microbiota and immune responses. For example, the gut microbiota can regulate lipid deposition through interactions with G-protein-coupled receptors (GPCRs) via short-chain fatty acids (SCFAs) and influence metabolic processes in the liver and adipose tissue, thereby indirectly affecting the risk of DN [36, 37]. The relationship between BMI and DN, and the roles of TG and TC, may therefore be influenced by these complex biological processes. These potential modulators may not have been fully considered or measured in different studies, leading to inconsistent results.
However, current research exploring the relationship between BMI, TG, TC, and DN has several limitations. Firstly, the lack of diversity in the study populations, particularly in terms of race and geographic location, limits the generalizability of the findings, making it challenging to apply the results to global populations. Additionally, potential modulators such as gut microbiota, immune responses, and endocrine dysfunction are often not adequately considered in existing studies, which may significantly affect the accuracy of the results. Moreover, there is a lack of in-depth investigation into the specific biological mechanisms involved, particularly regarding how elevated TG levels contribute to neural damage or how short-chain fatty acids (SCFAs) interact with G-protein-coupled receptors to regulate lipid metabolism and inflammation. Many studies rely on cross-sectional data, which limits the ability to establish causal relationships. Insufficient sample sizes and inappropriate statistical methods may also contribute to inconsistencies in the results. Despite the strengths of using large-scale GWAS datasets, our study is not without limitations. The reliance on secondary data sources introduces potential biases, including differences in genotyping platforms, population sampling methods, and phenotyping criteria across the datasets. Furthermore, GWAS-based MR studies are susceptible to horizontal pleiotropy, where genetic variants influence the outcome through pathways unrelated to the exposure. Although we conducted extensive sensitivity analyses, including MR-Egger and MR-PRESSO, to mitigate these biases, residual pleiotropy cannot be entirely ruled out. Additionally, the lack of individual-level data limited our ability to adjust for potential confounders, such as lifestyle factors and medication use, which may influence the observed associations.
The findings of this study have important implications for clinical practice and public health. The identification of BMI as a causal risk factor for DN underscores the need for targeted weight management interventions as part of comprehensive diabetes care. Incorporating BMI monitoring and management into routine clinical workflows could aid in early risk stratification and prevention of DN. On a public health level, campaigns promoting healthy lifestyles, including balanced diets and physical activity, may help reduce the prevalence of obesity and its complications, including DN. Furthermore, the results highlight the importance of integrating genetic risk profiling into clinical decision-making, enabling personalized interventions that address both metabolic and neuropathic risk factors. Future research should focus on translating these findings into actionable guidelines and evaluating their effectiveness in real-world settings.
留言 (0)