In this study serial repeated measures of anemia status are demonstrated to be associated with increased COPD morbidity, including worse quality of life, lower functional status by 6MWD, and higher rates of severe and moderate-to-severe exacerbations. Furthermore, participants with increasing risk of developing anemia over time demonstrated a more rapid decline in functional status, lung function, and symptom burden compared to those with stable or decreasing risk of anemia. Together these findings suggest that longitudinal anemia status may be a predictor of morbidity and disease trajectory in COPD, with potential to identify the COPD sub-population which may benefit from treatment of anemia, supporting the need for guidance in work up and management of anemia in COPD.
We present novel findings examining the relationship between anemia status and COPD outcomes by repeated-measures analysis, adjusting for key confounders including cardiovascular comorbidity and supplemental oxygen use, which corroborate prior studies examining a single measurement of hemoglobin and noted associations with COPD morbidity [4,5,6,7,8]. Our findings demonstrated that SGRQ and 6MWD, two outcomes that take into account functional limitations and quality of life that plausibly can be impacted by other comorbidities, were associated with anemia. Alternatively, this association may be explained by the fact that anemia, unless in a very severe range, could manifest as exercise intolerance and decreased quality of life without a direct impact of dyspnea or other respiratory symptoms. Specifically, oxygen carrying capacity is reduced with anemia which limits oxidative capacity in muscle, leading to reduced exercise capacity, physical activity and mobility. In addition, a recently published study on cause-specific mortality in COPDGene, a longitudinal cohort of tobacco cigarette users including those with COPD, highlighted the importance of respiratory quality of life not only as a determinant of all-cause but also respiratory-specific mortality [27].
Anemia was also associated with increased exacerbations, another important predictor of mortality in COPD. A few previous studies have demonstrated anemia to be associated with higher rates of severe exacerbations and COPD exacerbations requiring hospitalization [28, 29]. As a corollary, our group found that polycythemia is associated with a reduced rate of severe exacerbations despite polycythemic individuals having worse disease severity by FEV1% predicted and increased emphysema [6, 30]. This trend may be explained by hemoglobin’s role as the limiting factor for oxygen carrying capacity [31]. Although the models in this study adjusted for lung function and supplemental oxygen use, anemia may result in reduced reserve to handle COPD exacerbations due to lower capacity for oxygen delivery which may compound symptoms into a more overt exacerbation. Although reverse causality for the association between chronic conditions like anemia and COPD exacerbations cannot be excluded, given the consistent epidemiological evidence, anemia may be an important treatable risk factor for COPD exacerbations and hospitalization.
This study further explored longitudinal anemia status trends using anemia risk profiles which has not yet been studied in the COPD population. Participants with increasing anemia risk had evidence of worse COPD disease trajectory by multiple parameters even compared to individuals with a stable anemia risk profile, which included persistently anemic individuals. Thus, it may not be anemia per se but the development of anemia, represented by increasing anemia risk, that is more relevant to COPD disease trajectory. The profile of increasing anemia risk could represent subacute blood loss such as a gastrointestinal bleed leading to iron deficiency or a state of reduction in bone marrow function as can be seen in states of malnutrition. It may also represent a significant worsening of existing or new multimorbidity, for example a new malignancy, reflecting an overall adverse trajectory of health. In both situations there may be a greater effect on COPD disease trajectory compared to a state of stable anemia risk, often seen with anemia of chronic disease, where an individual may be chronically compensated for the anemic state and thus more protected against adverse outcomes.
This pattern is reflected in the varying approaches to treatment of anemia in other chronic diseases. In the heart failure population where anemia was similarly found to be associated with poor outcomes, recent studies have underscored of the importance of not only iron deficiency anemia but also iron deficiency irrespective of anemia status [32]. Clinical trials have shown improvement in symptom severity, exercise tolerance and reduction of hospitalizations among heart failure patients treated for iron deficiency with intravenous iron [33]. Targeting iron deficient patients even prior to development of anemia may be selecting for patients who have the profile of increasing anemia risk which is more likely to affect disease status and symptom burden.
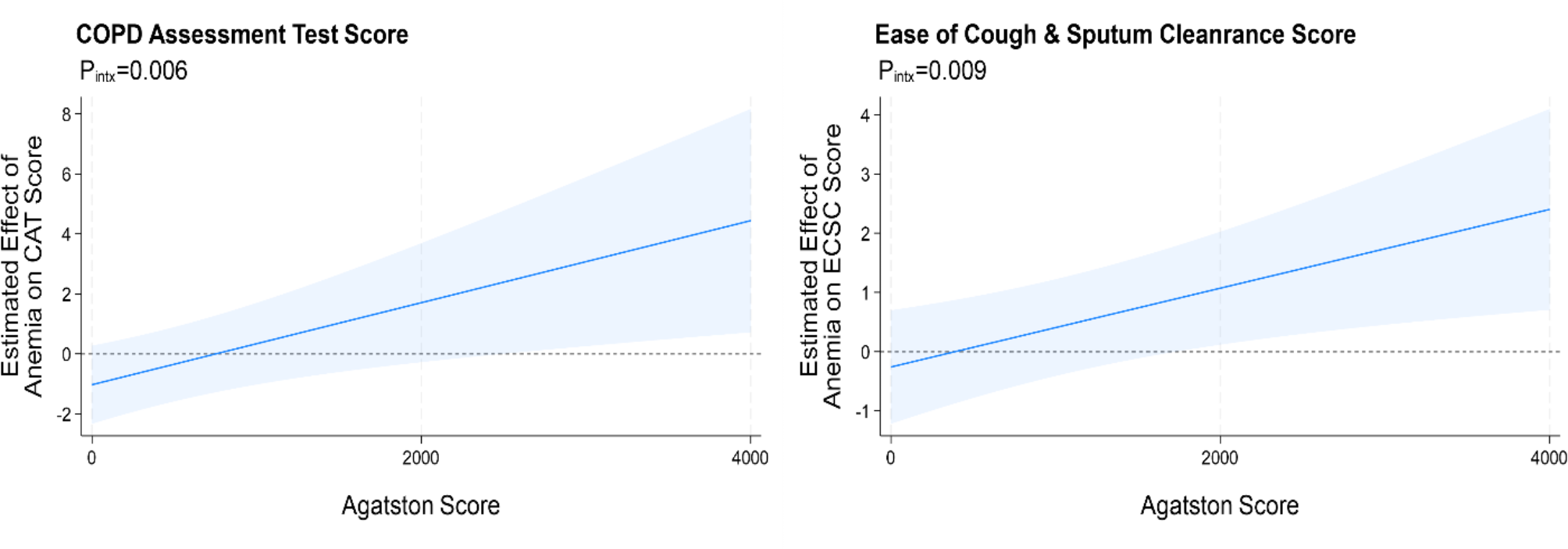
Finally, anemia and COPD do not co-exist in a vacuum but must be considered in the context of real-life COPD with multimorbidity and a high prevalence of cardiovascular comorbidities [1]. Yet the assessment of comorbid diseases in clinical studies remains challenging due to the reliance on participant self-report which, even when combined with medical record and medication review, are often discordant with diagnoses determined by objective disease criteria [34]. To overcome this, the Agatston score calculated from chest CTs provided an objective, graded measure of CAC burden which allowed for a more robust analysis to understand the presence of effect modification. Studies in the general population have shown an Agatston score of 300 to 400 is associated with an approximately five-fold increase in mortality compared to a score of 0 [35]. In COPD, CAC is more prevalent and the degree of CAC burden is greater, when compared with smokers with normal spirometry or non-smokers [36]. In this study, the statistically significant interactions between CAC and anemia were observed in the ranges of very high Agatston scores (≥ 2000) which may appear less clinically relevant. However, the Agatston score cut-off most predictive of the presence of CAD, myocardial infarction and heart failure (determined retrospectively) in a COPD population, has been suggested to be 1500 as opposed to 400, the accepted threshold defining severe CAC in the general population [37]. Of note, effect modification by CAC was limited to CAT scores and ECSC, which may be reflective of greater correlation of anemia, CAD, and respiratory symptoms in the chronic bronchitis COPD phenotype which is considered the more inflammatory sub-phenotype [38]. Overall, this analysis, while still exploratory with limited sample size, suggests that individuals with COPD with significant CAD based on high CAC burden may be a specific phenotype that can obtain greater benefit from treatment of anemia.
The associations of anemia, CAD, and COPD morbidity may be a manifestation of multimorbidity or driven by a unique causal mechanism. Prior work in the SPIROMICS observational cohort of individuals with COPD demonstrated that the effect of anemia on poor outcomes was independent of the impact of overall comorbidity burden, but the association between anemia and poor outcomes was stronger among participants with a higher burden of cardiometabolic comorbidities [5]. Further evidence that anemia is not just a marker of multimorbidity was shown in the study by Vanfleteren and colleagues which characterized clustering patterns of comorbidities in COPD including anemia. The comorbidity clusters revealed the prevalence of atherosclerosis was highest among individuals with anemia, but anemia tended to cluster in the “less-comorbid” group and did not correlate with the total burden of comorbidities [39]. Ultimately, while it is unclear whether this phenomenon reflects multimorbidity generally, the results underscore the potential value of screening for and treating anemia in COPD, given the evidence-based benefit of treating anemia and iron deficiency in conditions such as congestive heart failure which is similarly accompanied by a high comorbidity burden.
This present study has several limitations. First, this is a single center study comprised of two studies of former smokers with a relatively small sample size. This may limit generalizability of the results to the population with COPD actively smoking, have never smoked, or have different causative etiologies for COPD. Second, the study period was 6 to 9 months, a relatively short period for evaluation of trajectories, which does not allow for assessment of the importance of longer-term changes in anemia progression.
In conclusion, despite growing evidence of the importance of comorbidities in COPD outcomes and in understanding different COPD phenotypes, we lack evidence that could inform specific guidance for the approach to screening for and treatment of comorbidities in COPD. Our study adds to the growing evidence of the importance of anemia, specifically longitudinal anemia status, on COPD morbidity and disease trajectory. A greater understanding of the types of anemia as well as causal relationship between anemia and COPD outcomes will be necessary to elucidate the best approach to treatment. In the future, investigating the etiology of anemia in the COPD population in combination with longitudinal anemia status will help to identify patients who are both at risk for greater morbidity from anemia and thus may benefit the most from screening and treatment.


留言 (0)