Database
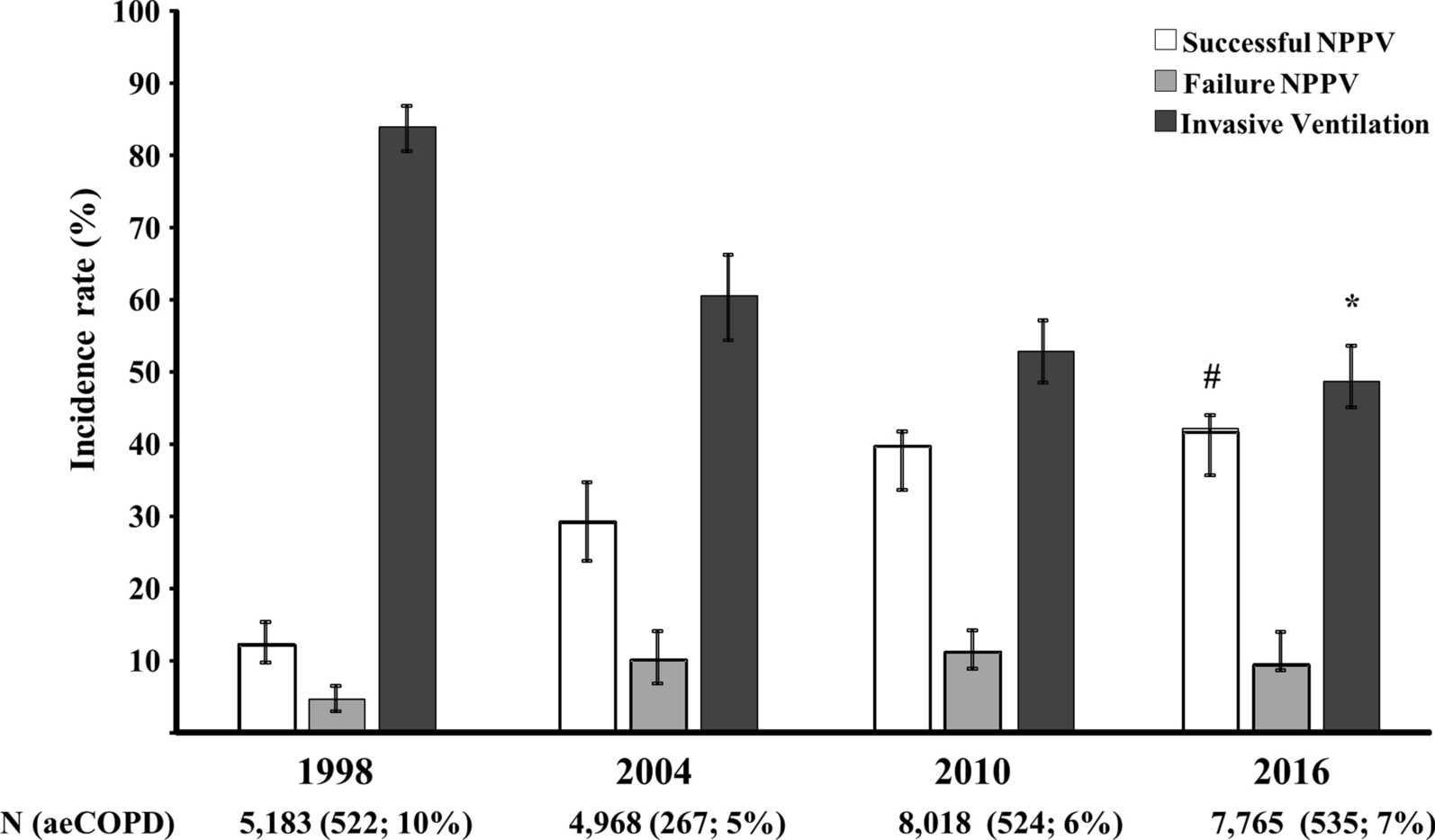
The study design was a retrospective analysis of the observational study performed by the International Study Group on Mechanical Ventilation [VENTILAGROUP] [15]. The VENTILAGROUP performed a prospective, observational, and multi-national study every 6 years from 1998, 2004, 2010, and 2016, from a total of 1253 units in 38 countries following the same methodology for each of the four studies, which included all critically ill adults, in a 1-month period, who received at ICU admission IMV longer than 12 h or NPPV for more than 1 h. The local practice of the ICUs participating in the study decided to use NPPV and initiate IMV. All studies collected data on baseline characteristics [age, gender, and severity at admission]. National coordinators from the participating countries recruited local investigators from eligible ICUs (see the complete list of Investigators in the Electronic Supplementary Material). Only the research team members at each site knew the purpose and the precise timing of the study. Ethics Committees of each participating institution approved the protocol; according to local regulations, the investigator obtained a waiver of informed consent.
Definitions
The definition of aeCOPD was pre-defined as the worsening of dyspnea and cough and sputum in the previous 14 days [17] in patients with a previous diagnosis of COPD and development of acute respiratory failure treated with ventilatory support either in the modality of NPPV or IMV at ICU admission. Patients with a history of COPD but who did not have acute respiratory failure due to their condition as the main reason for ICU admission were excluded.
We defined prolonged IMV as treatment with IMV for 14 days or longer [18], failure of NPPV as treatment with IMV after the delivery of respiratory support with noninvasive support [19], and lung protective ventilation strategy as tidal volume below 6 ml/kg predicted body weight or tidal volume below 8 ml/kg predicted body weight and plateau or peak inspiratory pressure less than 30 cm H2O [20].
Outcomes
The primary outcome was all-cause ICU mortality [21]. Prespecified secondary outcomes included ventilatory management during the first three days, failure of NPPV, complications during IMV up to a maximum of 28 days and only if they appeared 48 h after mechanical ventilation (barotrauma, acute respiratory distress syndrome (ARDS), ventilator-associated pneumonia (VAP), sepsis, cardiovascular dysfunction, acute renal failure, liver failure and coagulopathy), duration of ventilatory support, length of ICU stay, need of reintubation along the ICU stay, tracheotomy rate, hospital mortality and length of hospital stay.
For this study, the countries were grouped into six geographical regions: North America (Canada and the United States of America [USA], South America, Europe, Asia, Oceania (Australia and New Zealand), and Africa.
Individual countries were also classified into three income groups by their 2011 gross national income (GNI) per person, using thresholds defined by the World Bank Atlas method [22]: GNI less than US$4,045 as low and lower-middle income, $4,045–$12,535 as upper-middle income, and greater than $12,535 as high income, and then classified as follows: Low GNI countries: Bolivia, India, Morocco, Vietnam, Egypt, Tunisia; Lower-middle GNI countries: Argentina, Brazil, Mexico, Colombia, Ecuador, Guatemala, Peru, Venezuela, China, Turkey, Thailand; High GNI countries: USA, Canada, Australia, New Zealand, Spain, France, Germany, Greece, Italy, Chile, Korea, Portugal, Rusia, Uruguay, UK, Saudi Arabi, Ireland, Belgium, Denmark, Hungary, Netherlands, Panama, Poland, Puerto Rico.
Statistical analysis
The main objective of the analysis was to evaluate the inter-country variability over time of ICU mortality.
We summarized data with means and standard deviation (SD), medians and p25 and p75s, or numbers and percentages. Crude mortality rates are given as percentages with a Wald 95% confidence interval (CI). Single missing values were imputed by linear interpolation. When the first or last values are missing, carry the nearest value backward or forward.
We used the Kolmogorov–Smirnov test, histograms, and quantile–quantile plots to verify whether there were significant deviations from the normality assumption of continuous variables. We did different testing between groups with ANOVA, Kruskal–Wallis test, Student’s t-test, Mann–Whitney test, χ. Test, or Fisher’s exact test, as appropriate. The least significant difference testing procedure was used for pairwise comparisons.
ICU death was analyzed using multilevel logistic regression with three levels: patient, hospital, and country. We provide the results of fixed effects (measures of association) as odds ratios (OR) with their 95% CIs and the 80% interval OR. Random effects (measures of variation) measures included the variance and its standard error (SE), the proportional change in variance, and the median OR [23, 24]. We calculated the statistical significance of covariates with the Wald test.
The objectives of the analysis were to investigate the potential predictive model of three main outcomes: ICU mortality, failure of NPPV, and the need for prolonged IMV.
We performed logistic multivariable models to evaluate the prediction of failure of NPPV and ICU mortality. We evaluated the failure of NPPV only in those patients who received an initial attempt of ventilator support for a trial of NPPV at ICU admission. The variables included in this model were age, SAPS II, physiologic respiratory values (pH, PaCO2, PaO2/FiO2 ratio), and development of cardiovascular failure on day 1, defined as an increase in Sequential Organ Failure Assessment (SOFA) score higher than 2 points [25]. The ICU mortality was analyzed in all patients and adjusted by prespecified covariates as follows: age, SAPS II, gas exchange parameters on day 1 of ventilatory support (pH, PaCO2, PaO2/FiO2 ratio), cardiovascular failure on day 1, use of lung protective ventilator strategy on day 1.
We defined the outcome of prolonged IMV in three categories: patients who do not die and have a duration of IMV of less than 14 days, patients who do not die and have a duration of IMV longer than 14 days, and patients who die before 14 days. For this outcome, we performed a multinomial logistic regression. The variables included in the model were age, SAPS II score, variables within the first 72 h at admission in the ICU (PaO2/FiO2 ratio, cardiovascular failure, protective ventilation, barotrauma, ARDS complication, and VAP on day 3), and initial treatment with IMV at ICU admission.
To characterize country-level variation and estimate country-specific rates of ICU mortality, we fitted a mixed-effects logistic regression with a random effect in which the patients were nested in countries. If the patient was moved to an area with higher ICU mortality, we calculated the median odds ratio (MOR) to estimate the impact on the risk of death in the ICU [26, 27].
In all the models, we applied backward elimination of predictors from the full model with p-value < 0.05. We evaluated the discrimination of the model using the area under the curve (AUC). For the multinomial logistic model, we generate multiclass ROC curves for classification accuracy based on multinomial logistic regression using the “mlogitroc” command in Stata. We performed the analyses using Stata, version 17.0 (StataCorp LLC).


留言 (0)