
記住我
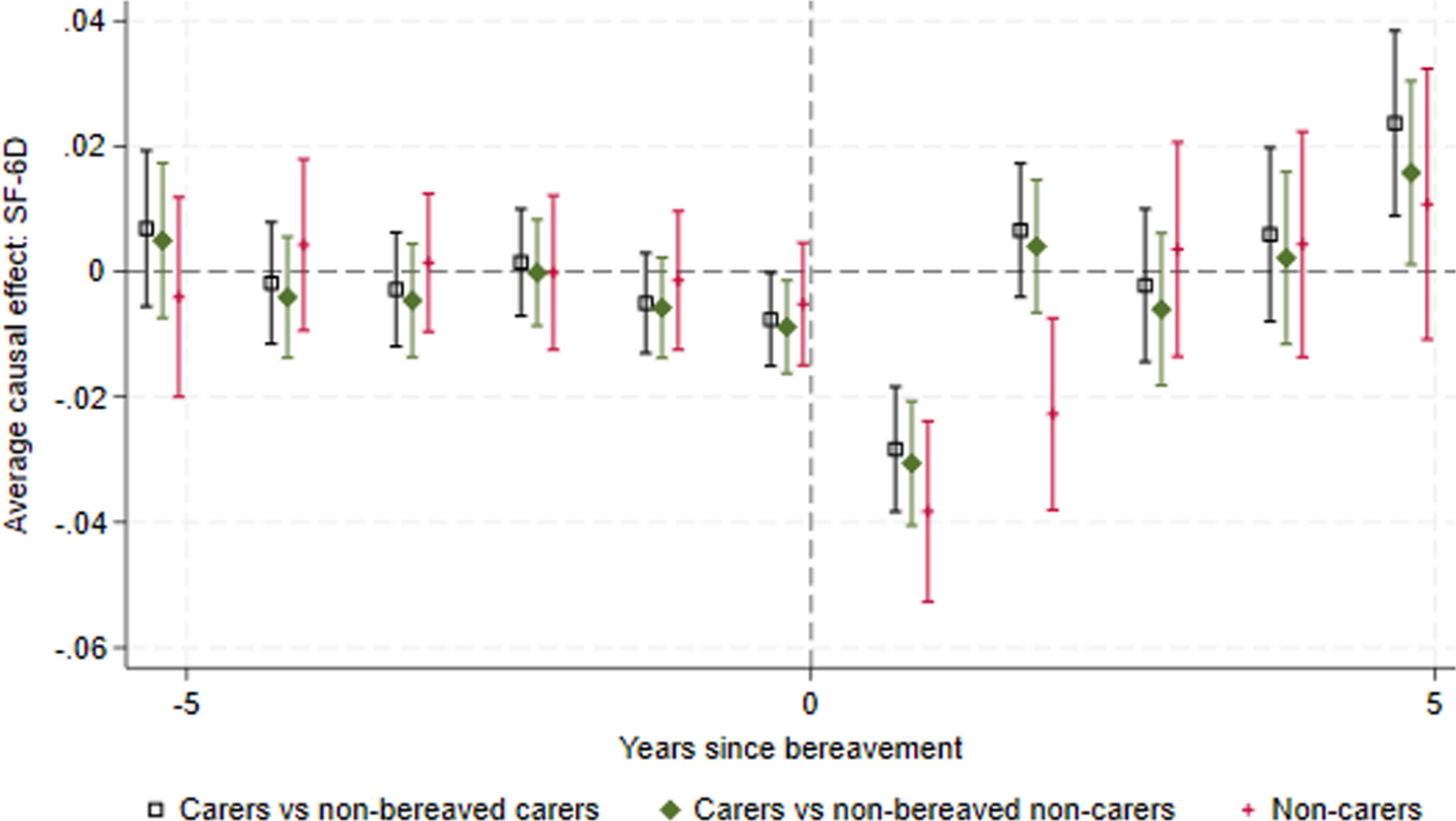
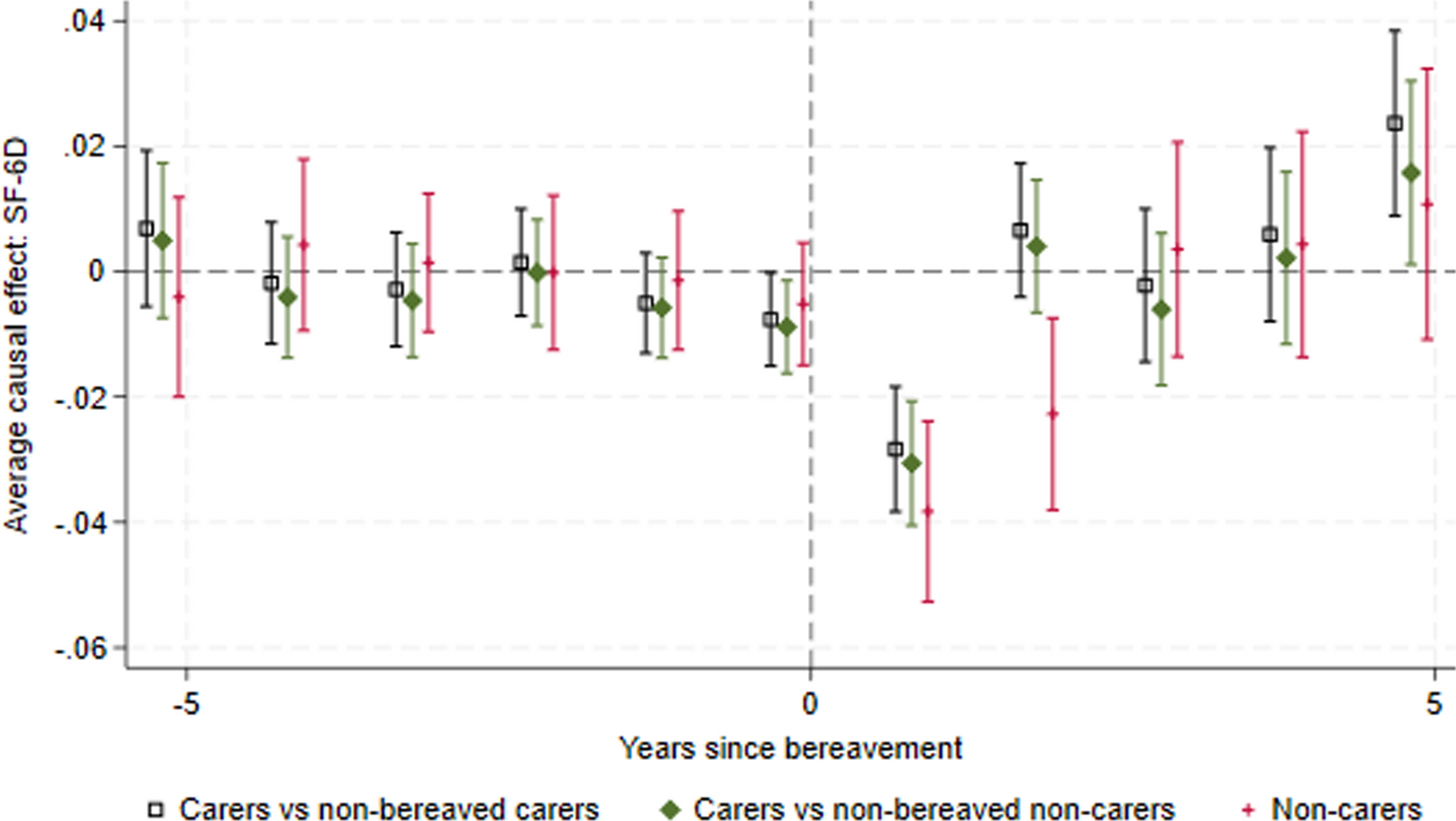

Table 1 shows the characteristics for carers and non-carers, who do and do not experience bereavement at first observation in the dataset. We note that these are not the baseline characteristics used in the analysis, where baseline is the period before treatment (bereavement) for the ‘treated’ (bereaved) population, and for the control group is the pre-period for the comparison at each given time. For example, for people who become bereaved at wave 2, the control group is people who have observations at both wave 1 and wave 2 and the baseline characteristics are those reported at wave 1. First observation characteristics are presented here to allow comparison of the populations and to identify characteristics which may differ at entry, and which may be expected to influence HRQoL trajectories.
Table 1 Baseline characteristics at first observation, unadjusted. Table presents number and (% percentage) or mean and (standard error)In comparing bereaved carers with non-bereaved carers, we note that those who are bereaved are on average older, more likely to be female, more likely to have no educational qualifications, have on average lower income, but have similar baseline HRQoL scores. In comparing bereaved non-carers with non-bereaved non-carers, we note that those who are bereaved are on average older, more likely to be female, and more likely to have no educational qualifications. Income, presence of long-standing illness and initial HRQoL scores were similar. In comparing bereaved carers with bereaved non-carers, we note that carers are older, have a lower income, more likely to have a long-standing illness, but have a similar sex distribution and baseline HRQoL score.
As there were differences in age, sex, education, income and presence of a long-standing illness, and these may influence future health and HRQoL, we controlled for these using IPW and OR. We assume that the parallel trend assumption holds, conditional on these variables.
Most people are bereaved by the death of a spouse, but this is slightly less likely for carers where the proportion whose parent died is higher. A small number of people were bereaved by the death of a child, and this was less likely for carers than non-carers.
Characteristics for the cared-for person are also shown where the carer only provides care to one person (the majority of carers). The cared-for people who died in the dataset were older at first observation (as expected with bereaved carers being older and most carers being bereaved by the death of spouse) and a higher proportion were male (as expected with most carers being female spouses). Surprisingly, the cared-for who later died had higher HRQoL scores at first observations. However, these tended to decline rapidly in the period immediately before death, as shown in Appendix Fig. S2 in the ESM.
The last recorded characteristics of the deceased are tabulated by whether they were cared for in Appendix Table S1 (see ESM). People who died after being cared for were on average older and had much lower HRQoL scores and notably worse physical health outcomes. The proportion of the deceased who were recorded as previously diagnosed with specific health conditions is presented graphically in Appendix Fig. S3 (see ESM), where we see higher prevalence of most diseases in the population who were cared for before they died.
Figure 1 presents the ATT for the SF-6D for each period before and after the event, where the event is bereavement (Appendix Fig. S4 in the ESM presents the full study duration). The plot presents three comparisons: bereaved carers versus non-bereaved carers, bereaved carers versus non-bereaved non-carers, and non-carers versus non-bereaved non-carers. Unadjusted results were also undertaken and can be found in Appendix Fig. S5 (see ESM). The findings were similar regardless of whether adjustment was included.
Fig. 1
Effect of bereavement on SF-6D. Carers 1 = bereaved carers vs non-bereaved carers. Carers 2 = bereaved carers vs non-bereaved non-carers (household members who did not report providing care)
3.2 Prior to the EventThere is some variation in the ATT before period 0, but the confidence intervals tend to span zero (no causal effect), suggesting that the parallel trends assumption holds prior to bereavement. The ATT for both bereaved carers compared with non-bereaved carers and bereaved carers compared with non-bereaved non-carers comparisons becomes negative at period 0—this may reflect anticipatory grief (grief experienced before the death of the cared-for, due to realising what is about to happen, preparing for life without the dying person, and feelings of freedom or isolation [26] ) or it may reflect the known HRQoL loss associated with caregiving as the proportion of carers caring is highest at this timepoint [27, 28].
The mean SF-6D loss in the period immediately before death is − 0.00762 (95% CI − 0.0151 to − 0.00173) for carers compared with non-bereaved carers and is slightly smaller and not statistically significant for non-carers (− 0.00518, 95% CI − 0.0149 to 0.00459). The caregiving burden also increases in the period immediately before death, with a higher proportion of carers reporting providing care in this period (see Appendix Fig. S6 in ESM). It is therefore unclear whether the decrease in SF-6D in this period is due to the increased caregiving burden or anticipatory grief. When we consider only co-resident carers and non-carers bereaved by the death of the same person (e.g., an elderly woman caring for her husband whose adult child lives in the same household and does not provide care), the SF-6D losses are more similar and confidence intervals overlap (− 0.0240, 95% CI − 0.0489 to 0.008 for non-carers and − 0.0312, 95% CI − 0.0583 to − 0.00424 for carers). This supports the theory that the HRQoL loss immediately before death is due at least partly to anticipatory grief since co-resident non-carers would also experience anticipatory grief but not the caregiving burden.
3.3 Short-Term Bereavement EffectsCarers (both comparisons) and non-carers experience a significant loss in HRQoL in the period (period 1) immediately following bereavement: carers: − 0.0283 (95% CI − 0.0432 to − 0.0134), non-carers: − 0.0383 (95% CI − 0.0527 to − 0.0239). The confidence intervals overlap, suggesting that the initial bereavement effect is not statistically significantly different for carers and non-carers. The losses are relatively small when compared with the disutilities associated with caring [27] or with adverse events, for example arising from cancer treatments [29], suggesting that the effect of bereavement on HRQoL is relatively minor. In a naïve comparison of SF-6D scores for the combined population of carers and non-carers before and after bereavement, the HRQoL loss is − 0.0327 (95% CI − 0.0395 to − 0.0260).
We explored the impact of using the General Health Questionnaire (GHQ); again, we found an anticipatory effect for carers, a statistically significant effect in the year immediately following bereavement for carers and non-carers, and that this effect was numerically greater for non-carers than carers. While the ATT for the carers groups is close to zero 2 years after bereavement, the bereavement effect for non-carers appears to extend into year 2. The GHQ, a broader measure of wellbeing, showed similar scores for carers and non-carers 2 years after bereavement, with all CIs spanning zero (see Appendix Fig. S7 in the ESM). This suggests that there may be a difference in the duration of the bereavement effect for carers and non-carers but that this is sensitive to the instrument used. The SF-12 Mental Component Summary (MCS) tells a similar story, with all groups having a similar and statistically significant decrease in the year immediately following bereavement, and the non-carers group having an effect extending into year 2 (see Appendix Fig. S8 in the ESM). The SF-12 Physical Component Summary (PCS) suggests that physical health improves after bereavement (see Appendix Fig. S9 in the ESM), but we urge caution in interpreting this as the scoring system for PCS has negative coefficients for the questions related to mental health meaning that a decrease in mental health leads to an improvement in PCS, ceteris paribus [30].
3.4 Long-Term Bereavement EffectsThe results suggest that there is no sustained effect on HRQoL beyond 2 years after bereavement. The CIs for the ATTs for all groups tend to span zero, but we note that there is some variation likely due to low numbers of observations as the years since bereavement increases. It is notable that the bereaved carers versus non-bereaved carers mean is generally above zero and the bereaved carers versus non-bereaved non-carers mean below zero until year 5—this suggests that bereaved carers’ HRQoL may increase compared with providing ongoing care for a surviving patient.
3.5 Comparison of Bereavement Effects for Carers and Non-CarersWe compared the effect sizes at year 1 after the event from the Group 1 and Group 3 Difference-in-Differences where the confidence intervals (CI) overlap. At year 2, the effect for carers is non-significant: 0.00659 (95% CI − 0.00405 to 0.0172) and for non-carers is − 0.0227 (95% CI − 0.0380 to − 0.00741). We concluded that there are no statistically significant differences between the bereavement effects for carers and non-carers in the first year, and that there is a trend for a prolonged bereavement effect for non-carers in year 2 but the confidence intervals overlap.
3.6 Mechanism/Domains of SF-6DThe questions that seem to exhibit the biggest change after bereavement are 4a (emotional problems have caused problems accomplishing work or other regular activities), 6c (feeling downhearted or depressed) and 7 (physical health or emotional problems interfered with social life). The proportion of people answering in each category to these questions before and after bereavement are shown in Fig. 2.
Fig. 2
Responses to SF-6D domains for mental health, feeling downhearted and depressed, and social life, by time to bereavement for bereaved non-carers and bereaved carers
For each of these domains, in the period immediately following bereavement there is a reduction in the proportion of patients reporting the higher (better) scores and an increase in the proportion reporting lower scores. For bereaved carers, the effect appears to last only 1 year, whereas for non-carers the graphs suggest it may take 2 years after the event for the proportions to return to the pre-event trend. This corresponds to the non-significant negative ATT in period 2 for bereaved non-carers in Fig. 3, compared with the non-significant positive ATT in period 2 for bereaved carers in Fig. 1.
Fig. 3
Effect of bereavement on SF-6D, comparing bereaved carers with not-yet-bereaved carers, and comparing bereaved carers with not-yet-bereaved non-carers
There appears to be almost no change in 3b (physical health limiting kind of work), 5 (pain interfering with work), 6b (having a lot of energy) and only a small change in 2a (health limiting moderate activities) (see Appendix Fig. S10 in the ESM).
It appears to be the mental health/emotional impact of bereavement that is driving the change in HRQoL rather than physical health.
3.7 Comparison With Not-Yet-BereavedFor carers, there is no statistically significant anticipation effect (− 0.00635, 95% CI − 0.0155 to 0.00278) and the short-term bereavement effect is − 0.0252 (95% CI − 0.0369 to − 0.0135) in the first year. For non-carers, the short-term bereavement effect is − 0.0416 (95% CI − 0.0608 to − 0.0225), and the effect is not statistically significant beyond the first year. The trends and effect sizes are similar to the never-treated comparison, but the sample sizes are smaller and so the confidence intervals are wider. The graph is presented in Fig. 3.
3.8 Subgroup Analysis3.8.1 Alternative Carer PopulationsIn the population where carers must have reported providing care before their baseline for the control group, the trends and effects sizes were similar to the base case, but the confidence interval increased, due to the reduced sample size (Appendix Fig. S11, see ESM). The same was true for the subgroup of carers who provided care only to one household member (Appendix Fig. S12).
3.8.2 SexIn the subgroup analysis in Fig. 4, it is notable that female non-carers have the greatest HRQoL loss in the first two periods after bereavement. Male non-carers have the smallest HRQoL loss initially. Male carers appear to experience the greatest anticipation effect. This may suggest that males and females are affected differently by bereavement, and that the impact of caring on the bereavement effect may differ by sex. However, the confidence intervals tend to overlap, suggesting these differences are not statistically significant.
Fig. 4
Effect of bereavement on SF-6D for subgroups based on sex and caring status
3.8.3 RelationshipWhen we examine the relationship of the bereaved to the deceased (including carers and non-carers combined), the HRQoL loss appears to be largest for spouses, while the effects for (adult) children whose parents die are smaller (Fig. 5). The HRQoL change for parents whose children die are not significant, due to the much smaller sample size (n = 47) and outcomes for this group are highly uncertain. We found similar results using the GHQ (see Appendix Fig. S13 in the ESM). The last recorded characteristics of the deceased person are tabulated by relationship in Appendix Table S2 (see ESM).
Fig. 5
Effect of bereavement on SF-6D for subgroups based on the bereaved person’s relationship to the deceased
3.8.4 Age at DeathIn Fig. 6, we show the effect of the age at which the deceased died on the bereaved person’s HRQoL changes. The point estimates for the effect sizes generally appear to be smaller when people die aged 80+ years than when they die aged 60–79 years, but the confidence intervals generally overlap. The effect size for when people die aged under 50 years or 50–59 years are similar to each other and the other age groups in the first year after bereavement. In the second year after bereavement, the effect size appears bigger where people died aged under 50 years (but still less than −0.05 and not statistically significantly different to where people died aged 60–69 years) and smaller where people died aged 50–59 years. By 3 years after bereavement, the effect sizes appear similar regardless of the age at which the deceased died. We note that the confidence intervals are wide for the younger ages as there are fewer deaths at these ages (see Appendix Fig. S14 in the ESM).
Fig. 6
Effect of bereavement on SF-6D for subgroups based on the deceased person’s age at death
留言 (0)