
記住我

A cross-sectional, web-based DCE survey was used in this study. The study design and reporting of this DCE were based on the guidance of a DCE user’s guide and two reports from the ISPOR Good Research Practices for Conjoint Analysis Task Force [16,17,18]. The University of Utah Institutional Review Board (IRB) approved this study (IRB-00147477) to be exempt from human subject review.
2.1 Identification and Selection of Attributes and LevelsFirst, a systematic literature review (SLR) was conducted to develop a list of MM treatment attributes (i.e., efficacy, safety, administration and/or convenience, innovation, and cost) that are likely important to patients with MM and HCPs, and their levels. This list was used to guide two semistructured focus group discussions (FGDs) with ten English-speaking patients with MM and in-depth interviews with five HCPs involved in MM care between October and November 2022 to determine important MM treatment attributes. Of the ten patients participating in the FGDs, two were African American, one was Asian, and the others were white, and two were newly diagnosed and aged below 50 years. For the in-depth interviews, HCPs, who were involved in the patients’ decision-making processes, namely physician–oncologist, nurse practitioner, and clinical pharmacist, and had a minimum of 1 year of experience providing MM care, were included. From these qualitative approaches, two innovation attributes of MM treatments, including the opportunity to live without MM treatment and scientific innovation, were consistently identified by both patient and HCP groups. At the end of the interviews, patients and HCPs were asked to rank the importance of the discussed attributes. Finally, the study team members, consisting of clinicians, DCE experts, and health outcomes researchers, reviewed the evidence in the SLR and interviews, as well as the latest clinical trials and emerging therapies. Through various rounds of discussions and consensus meetings, the study team systematically assessed the relevance and clinical significance, and primarily based the decisions on the findings from the patient interviews to ensure that the selected attributes were potentially important to patients with MM. The final list of five attributes, with distinct levels, was developed through this approach (Table 1): (1) progression-free survival (PFS; 6, 12, 24, 48 months), (2) chance of severe side effects (5%, 10%, 20%), (3) how patients live with MM treatments (living without treatment; living with treatment at home; living with treatment at a hospital/clinic), (4) scientific innovation, defined as a treatment that either is first-in-class or leads to the development of better MM treatments (yes, no), and (5) monthly out-of-pocket (OOP) cost ($100, $500, $1000, $1500). The attribute levels of PFS, chance of severe side effects, and OOP cost were derived from the SLR findings, while the levels of the other two attributes, i.e., how patients live with MM treatments and scientific innovation, were obtained from the results of the focus group interviews with the patients, followed by the discussion among the study team members, including an MM specialist physician.
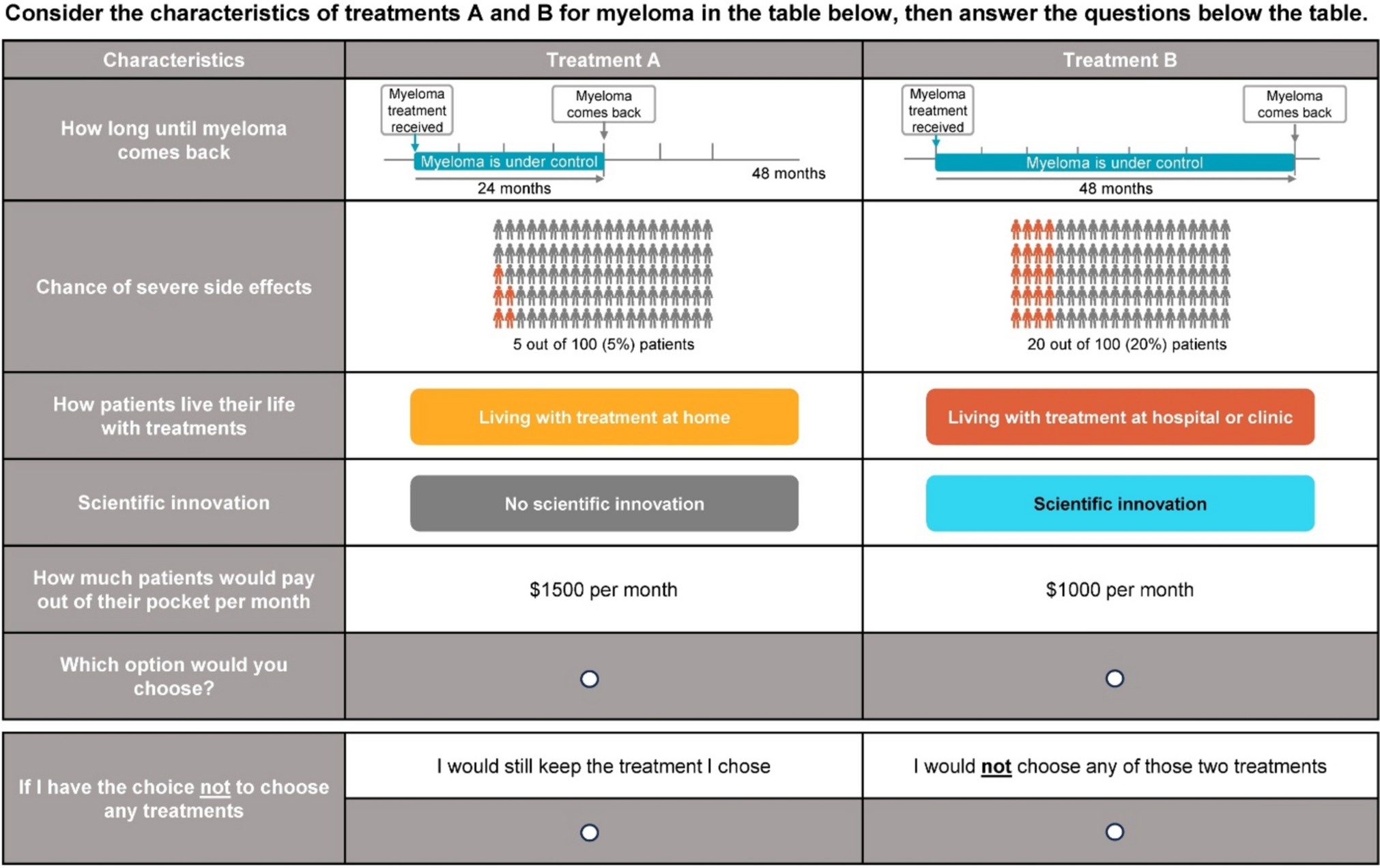
Table 1. Treatment attributes and levels included in the discrete choice experiment2.2 Survey DevelopmentA DCE was utilized to estimate the value that patients and HCPs placed on the attributes and associated attribute levels of MM treatments. Following the selection of attributes and their levels, a full-length survey was developed, incorporating a D-efficient DCE survey design created using Ngene® software (ChoiceMetrics, version 1.2). The design included six blocks, each including six choice sets, resulting in a total of 36 profiles. Each block contributed to one unique version of the survey. Each choice set included two unlabeled hypothetical MM treatment alternatives described by the selected attributes and their levels. In each choice set, participants were requested to choose a preferred alternative, followed by an option to opt out of the treatment. Before participants responded to DCE questions, detailed descriptions in plain language and graphics of the attributes, as well as practice questions, were provided to ensure their understanding and minimize bias. To ensure the quality of responses, one validity choice set, consisting of a repeated choice set, was included in each survey version, resulting in seven choice sets per patient. The content of the survey was validated by a clinical expert and a survey expert. Then, the survey was validated with five patients using the think-aloud method [19], with each session lasting approximately 1 h. During these sessions, patients were instructed to think out loud while completing the survey. On the basis of their feedback, the survey was modified and then piloted with 30 patients with MM. This pilot study was designed to further explore results and confirm whether the survey questions and choice experiment performed as intended [19]. It also generated prior parameters to inform a Bayesian-efficient design with four blocks, each including nine DCE choice sets in the main survey. In the main survey, two validity choice sets, consisting of dominant and repeated choice sets, were included in each survey version to ensure the quality of responses, resulting in 11 choice sets per patient or HCP (an example choice set is presented in Fig. 1). Questions about the demographic characteristics of patients or HCPs were included in the surveys. Questions on patients’ experience with MM (e.g., relapse experience, stem cell transplant experience) or HCPs’ experience treating patients with MM (e.g., the number of patients with MM seen per week) were also included in the surveys.
Fig. 1
Example choice set. Patients and HCPs were asked to choose the preferred alternative from a set of two hypothetical MM treatment options. Each alternative was described by a selected attribute and their levels to analyze patient and HCP preferences. HCP healthcare provider, MM multiple myeloma
2.3 Inclusion Criteria and Data CollectionTo be included in the patient survey, the following eligibility criteria were required: (1) diagnosed with MM by a physician, (2) aged 18 years and above, (3) proficient in English, and (4) residing in the USA. To be included in the HCP survey, an individual must be a physician, pharmacist, or nurse in the USA who provided care for patients with MM and was involved in and influenced patients’ treatment decisions. Survey participants were recruited between March and August 2023 by Global Perspectives (GP), a research firm based in the UK, using online panels, patient databases, social media, and advertisements. While a convenience sampling technique was used, GP was asked to ensure a good representation of US patients as reported in a national database such as the Surveillance, Epidemiology, and End Results database in terms of sex, race/ethnicity, insurance status, and geographical region. HCPs were purposely selected to include physicians, nurses, and pharmacists. By Orme’s rule of thumb, the minimum sample size of patients required for this study is 91 [20]. Additionally, upon consideration of the estimated sample size and other strategies, which included the ISPOR good research practice report [21] and a published practical guide [22], we targeted to include a minimum of 160 patients with MM for the patient survey. Owing to limited resources, this study targeted 30 HCPs, which should be sufficient on the basis of the research team’s previous DCE experience in treatments for another type of oncology disease state [23]. Both patient and HCP surveys were self-administered on a web-based platform. Each participant was randomized to one of the four survey versions.
2.4 Data AnalysisOnly responses from the participants who passed the validity choice sets were included in the analysis. Patients’ and HCPs’ sociodemographic characteristics and experiences with MM were descriptively analyzed. Summary statistics, including mean and standard deviation (SD), or median and interquartile range (IQR), are reported for continuous variables. For categorical variables, frequencies and percentages are reported. On the basis of random utility theory, responses for each choice set were analyzed using a mixed logit (ML) model to determine the perceived value of an alternative with the utility function (Unsj) for participant n with a choice set s and an alternative j, where only main effects were included. All variables were assumed to be categorical, and effect coding was used:
$$ \begin U_ & = \beta_ + \beta_ }1_ + \, \beta_ }2_ + \, \beta_ }3_ \\ & \quad + \beta_ }1_ + \, \beta_ }2_ + \, \beta_ }1_ \\ & \quad + \, \beta_ }2_ + \, \beta_ }1_ + \, \beta_ }1_ \\ & \quad + \, \beta_ }2_ + \, \beta_ }3_ + \varepsilon_ , \\ \end $$
where β0 is the constant reflecting the preferences for choosing the two treatment alternatives, instead of the opt-out alternative. βn1, βn2, βn3,…. βn11 are the coefficients or preference weights of the effect codes of the PFS, the chance of severe side effects (SSE), how patients live their life with treatments (LWT), having scientific innovation (SI), and the OOP cost per month (Cost), respectively. εnsj is the error term. The means and SDs of all preference weights were estimated using the maximum simulated likelihood method with 1000 Halton draws. A Wald test was used to evaluate whether there was a difference between the preference weights of two adjacent levels of the attributes. The estimated preference weights were then used to calculate the conditional relative importance of attributes. First, the range of attribute-specific levels was calculated by measuring the difference between the highest and lowest preference weights for the levels of the respective attribute. The conditional relative importance was then calculated by dividing the range of the attribute-specific levels by the sum of all attribute level ranges. All analyses were performed separately for patients’ and HCPs’ survey data. Additionally, a sensitivity analysis was performed including both valid and invalid responses.
Given the potential of preference heterogeneity across patients, a latent class model was developed to classify patients into distinct subgroups (or latent classes), each having a similar pattern of preferences for MM treatments. Up to six classes were fit to determine the optimal number of latent classes with the main effects. The model with the minimum Bayesian information criterion values was selected as the final latent class model. P value less than 0.05 was considered statistically significant. All analyses were performed using STATA version 17.0 (StataCorp 2021, College Station, TX, USA).
留言 (0)