To our knowledge, this work, utilizing the CHARLS database, is the sole study that examined the prevalence of headaches and their associated risk factors in middle-aged and elderly stroke patients in China. According to 2018 data, stroke patients exhibited a markedly higher prevalence of headaches compared with nonstroke patients. Regardless of stroke occurrence, the prevalence of headaches exhibited significant differences in terms of gender, education level, ethnicity, geographic distribution, health status, shoulder pain, chest pain, back pain, night sleep duration, and hip pain. This study is the first to document the prevalence rate of headaches among middle-aged and elderly stroke patients in 2018. In addition, according to multivariate logistic regression, the risk factors for headaches in stroke patients include female gender, residency in Central, Eastern, or Northwestern China, poor and very poor self-reported health status, diabetes, shoulder pain, back pain, and chest pain.
Overview of disease prevalence
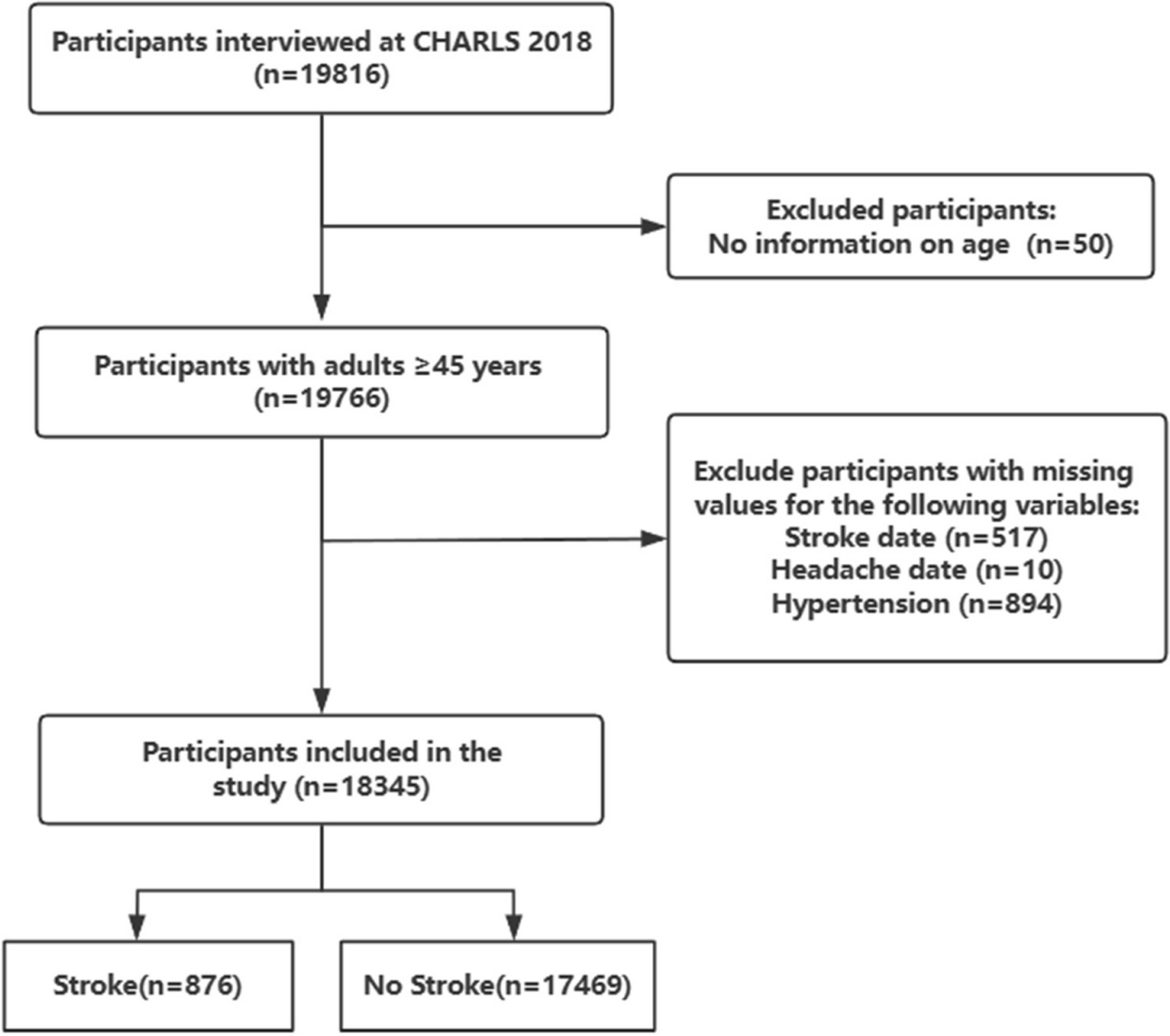
This research involved 18,345 participants, among whom 328 and 4,249 stroke and nonstroke patients, respectively, experienced headaches. Our analysis of the 2018 data revealed that the prevalence of headaches among stroke patients in China who are middle-aged and older reached as high as 37.44%, which indicates an epidemic level, consistent with the range reported in previous studies [19]. The prevalence of headaches in nonstroke patients was 24.32%, with a significantly high correlation observed between headache occurrence and stroke incidence [20]. Moreover, accumulating pieces of evidence suggest a common genetic basis between headaches and vascular diseases [21]. In cases of posterior circulation ischemic stroke, headaches are more common. Cerebrovascular diseases can simultaneously cause stroke and headache disorders, such as cerebral venous thrombosis [22]. Headaches often present as prodromal symptoms, and early intervention is crucial to prevent serious consequences.
Stratified analysis was conducted based on sociodemographic information and health-related data. Notably, women exhibited significantly higher stroke prevalence than men; based on earlier research, female stroke patients had a 2.06-fold higher likelihood of experiencing headaches than their male counterparts [23]. Furthermore, environmental factors and physical fitness may influence changes in headache prevalence, and chronic diseases, such as diabetes, increase the likelihood of headaches. The high prevalence observed in ethnic minorities may be attributed to regional and dietary factors, with low levels of cultural awareness potentially contributing to the increased prevalence of headaches because of factors, such as overwork, irregular sleep patterns, and inadequate rest [24]. A high prevalence of headaches was also observed in individuals with poor health conditions. Such an outcome was observed because psychological factors affect self-reported health status, and an improved mental state can regulate peripheral nerves, endocrine functions, and immune factors to alleviate pain [25]. Conversely, a poor psychological state exacerbates headaches through the manifestation of a poor reported health status. Nondrinkers exhibited a higher headache prevalence than drinkers, possibly because patients experiencing headache symptoms may abstain from alcohol consumption to mitigate the exacerbation of their headaches [26]. Conversely, nonsmokers presented a higher prevalence rate of headaches than smokers, potentially because smoking helps in the management of emotional pain [27]. However, given the limitations inherent in cross-sectional studies, establishing causality between smoking and headaches remains challenging. Future research should conduct longitudinal studies to further investigate the causal relationships between smoking, alcohol consumption, and headaches to develop targeted interventions.
Overview of risk factors
The findings reveal that the female gender, residency in central, eastern, or northwestern regions of the country, poor self-health, having diabetes, and shoulder pain, back pain, or chest pain were risk factors for headaches in stroke patients. The likelihood of suffering from a headache is notably greater in women than in men [28, 29]. This outcome may be explained by the hormonal and physiological control of proteins in females, whereby a reduction in estrogen levels may cause the upregulation of the sympathetic nervous system and downregulation of serotonergic system to be [29]. In addition, females are more susceptible to emotional fluctuations and may bear higher psychological and physiological burdens, such as depression and anxiety, compared with males. Therefore, targeted attention must be focused on the female population experiencing headaches among stroke, and relevant interventions must be offered to mitigate risk factors.
Previous studies have indicated that individuals facing economic challenges are prone to headaches. The central and eastern regions of China, which are relatively developed economically and predominantly urban, may harbor headache risk factors associated with adverse lifestyle factors, such as stress and insufficient physical activity [30]. By contrast, in regions such as the northwest, which may be characterized by relative economic underdevelopment and the lack of adequate medical environments and infrastructure, headache prevalence among stroke patients can be influenced. Moreover, abundant sunlight exposure may contribute to headache occurrence [31], which can also be affected by the participants’ own physical conditions and the location of stroke lesion.
A poorer self-reported health status serves as a risk factor for headaches, and it indicates a higher awareness of self-health among individuals compared with those reported in previous studies; this finding suggests an increased self-awareness compared with those in past research [32]. Our study revealed an association between diabetes and headaches in stroke patients and an association between headaches and cardiovascular risk factors, including type 2 diabetes [33]. Common chronic conditions, such as diabetes, can increase the prevalence of headaches in stroke patients [34]. Shoulder pain ranks among the most prevalent neuropathic pain syndromes following a stroke [35]. Typically, the effects of stroke manifest on one side of the body, and a mutually exacerbating relationship exists between headaches and shoulder pain [36]. Previous studies have shown a positive correlation between lower back pain and headaches, which may be attributed to diminished dopaminergic effectiveness or deficiencies in emotional awareness. This correlation may also be linked to the calcitonin gene-related peptide in biology, which functions as a neural modulator for pain syndromes other than headaches [37]. Most patients with ischemic heart disease experience chest pain. Research indicates that rare cardiac-origin headaches can also lead to headaches. Chest pain may arise from conditions, such as angina, that can increase intracardiac pressure and trigger the release of atrial natriuretic peptide. This release, in turn, can cause vasodilation of cerebral blood vessels, which leads to headaches [38].
In stroke patients, those without hypertension, smoking, or alcohol consumption shows a higher prevalence of the disease than those with such risk factors. Consequently, in the analysis of the risk factors for headache, we excluded smoking, alcohol consumption, and hypertension due to the small sample size of stroke patients. Age emerged as a protective factor in the multivariate analysis of logistic regression. In addition, the frequency of headaches associated with stroke declines with advancing age, which is in line with earlier findings [34, 39, 40]. However, other research indicated that the highest prevalence can be observed among those aged ≥ 55 years, followed by those aged ≤ 18 years [23]. Therefore, we also excluded the controversial age factor in our logistic regression analysis. The findings revealed that residential area, diabetes, and self-reported health status are modifiable risk factors for headaches in stroke patients.
Strengths and limitations
This study exhibited several notable strengths. Primarily, this work leveraged data sourced from the 2018 CHARLS survey. The participants were selected via a rigorous multistage probability sampling procedure, which guaranteed the efficient representation of a middle-aged and older population sample that is nationally representative. Second, this study, which was conducted through a cross-sectional study design, presents the first targeted assessment of the prevalence rate and risk factors associated with concurrent headaches in patients who suffered from stroke. Ultimately, this study established a foundation for providing stroke patients with insights into modifiable risk factors linked to the occurrence of headaches and their potential complications and the development of preventive policies.
The study encountered several limitations. First, given its cross-sectional design, the causal relationships between headaches among stroke patients and their associated risk factors was not established in this work. Second, the study relied on retrospective data reporting, which might have introduced sampling bias toward patients with mild strokes and those with adequate communication abilities, as well as being influenced by respondents' memory bias, potentially reducing the precision of the results. Third, the data did not provide detailed classifications of stroke and headache types or severities, which limits the generalizability of the study’s findings to populations meeting more specific stroke criteria. Future research should incorporate objective clinical data to address the limitations of self-reports and further investigate the prevalence and risk factors of headaches in populations with varying stroke types and severities. Additionally, the over-representation of headaches in the stroke population may partly reflect the increased stroke risk in patients with migraine. This phenomenon warrants further investigation to determine whether headaches are a direct consequence of stroke or a manifestation of other comorbid conditions. Lastly, based on the available medical history, we cannot determine whether the headache was caused by the stroke. Moreover, the questionnaire did not assess whether the headache meets the definition according to ICHD-3 criteria. Future research should employ prospective cohort studies combined with the internationally standardized ICHD-3 diagnostic tool to further investigate the relationship between headaches and strokes.


留言 (0)