Route
Both the Neurocritical Care Society and the American Heart Association/American Stroke Association guidelines support the use of the oral or enteral route for nimodipine administration [4, 5], based on historical RCTs performed decades ago [10, 11].
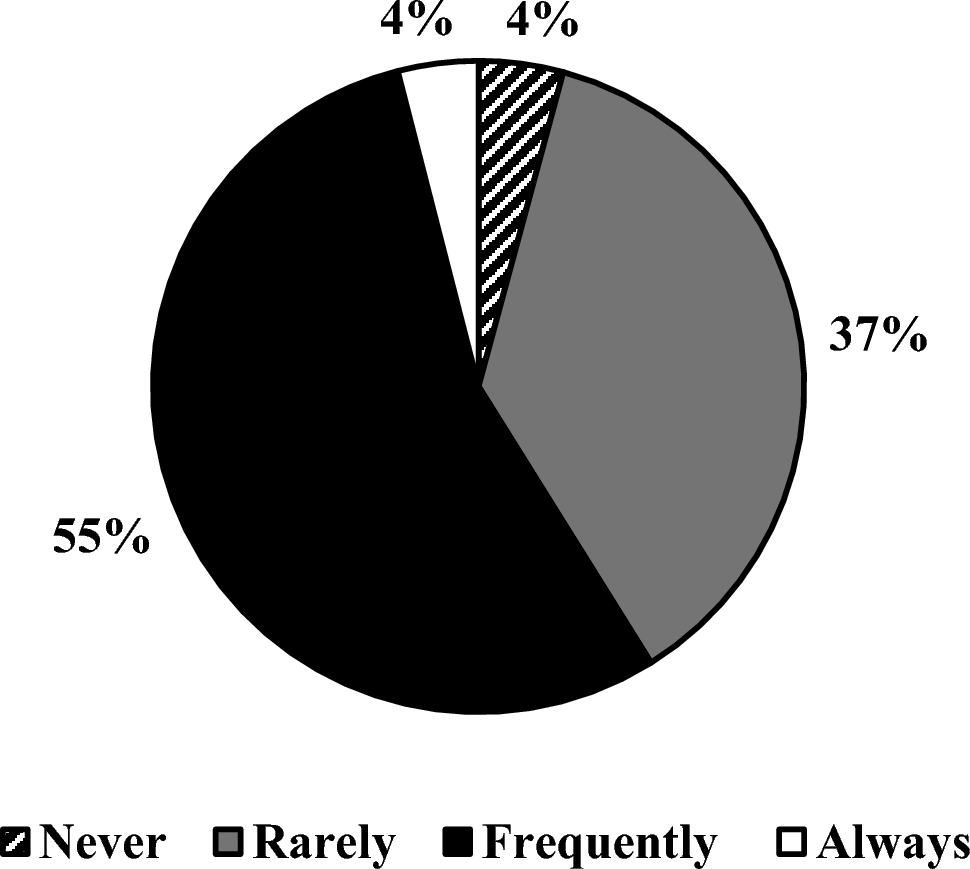
According to the MANTRA survey, up to 71% of the respondents used the oral or enteral route, 9% used the intravenous route, and 20% used both [3]. The use of the intravenous route has been questioned because of a higher risk of arterial hypotension [12,13,14]. Recently, Rass et al. [12] showed that given in the oral or enteral form, hypotension affects 1 of 10 patients compared with 1 of 3 patients when using the intravenous formulation, supporting previous investigations [13, 14]. Hypotension and blood pressure variability is associated with poorer outcomes in patients with aSAH, according to observational data [15].
However, taking nimodipine with meals results in a decreased peak plasma concentration and lower bioavailability compared with fasting [7], which is troublesome in the neurointensive care unit. In addition, a recent multicenter study showed that enteral nimodipine formulations and administration techniques might not be equivalent, a fact that could be attributed to excipient differences, inconsistency and inaccuracy in medication administration, and altered nimodipine bioavailability [16]. Therefore, oral and enteral forms might not be interchangeable because oral nimodipine is in the form of capsules and enteral administration can be via prefilled syringes or extracting it from capsules [16]. Furthermore, in some countries, nimodipine is in the form of tablets, and the pharmacokinetics of tablets is not the same as capsules, at least in healthy human volunteers.
Additionally, recent meta-analyses showed that both routes can be effective in preventing poor outcome, DCI, and neurological deficit [17, 18], but these meta-analyses are limited by the low number of studies evaluating intravenous nimodipine. Given that hypotension remains the major concern with the intravenous route (although nimodipine concentrations should be less variable because of no food-pass and first-pass effects compared with oral or enteral formulations), and the increasing use of minimally invasive or invasive cardiovascular monitoring in patients with aSAH may increase safety and potentially improve outcomes of the intravenous route [19], the authors believe that there is still space for RCTs comparing the oral and enteral routes with the intravenous route. It has to be noted that the vehicle in the original intravenous nimodipine formulation is almost 25% ethanol, so it can be vein-irritating and therefore has to be administered through a central venous catheter. A newly developed intravenous formulation of nimodipine using nonionic surfactant micelles as the drug carrier to solubilize nimodipine (without high ethanol concentrations) is currently being investigated in an industry-sponsored RCT (NCT05995405), but results are not yet available.
Another potential route using nimodipine consists of the intraarterial route. Intraarterial spasmolysis with nimodipine has been commonly used in patients with DCI as an option of treatment in patients who did not respond to induced hypertension [3, 20]. However, this is not free of complications, especially on blood pressure, with the need to increase vasopressor requirements to maintain induced arterial hypertension. To minimize this complication, Weiss et al. [21] demonstrated that a modified protocol including intraarterial spasmolysis with nimodipine allowed lower blood pressure targets with similar results. Of note, Vossen et al. [22] showed that long-term outcomes could be favorable in almost half of these patients treated with rescue intraarterial spasmolysis.
Additionally, intraventricular administration of nimodipine has been evaluated. An initial phase I/IIa study determined the maximum tolerated dose of intraventricular sustained-release nimodipine in aSAH. The maximum tolerated dose was 800 mg. There was no intraventricular nimodipine–related hypotension compared with 17% (3/18) with enteral nimodipine [23]. The follow-up study, the NEWTON RCT, evaluated the use of single-dose intraventricular (600 mg) sustained-release nimodipine microparticles (EG-1962). However, after an interim analysis of 210 patients with 90-day outcome, the trial was stopped early for futility in terms of clinical outcomes, despite the EG-1962 group having a lower incidence of angiographic vasospasm, DCI, and rescue therapy [9].
Dosing and Interval
Oral or enteral nimodipine at a dosage of 60 mg every 4 h for a duration of 21 days is the most commonly administered regimen in daily practice [5]. It must be pointed out that there is no dose–response evidence for this nimodipine dose-outcome relationship. Higher dosages (90 mg every 4 h) were associated with a higher number of patients with good recovery but also with a nonsignificant higher 3-month mortality (47.2% in the nimodipine group vs. 39% in the placebo group) [24]. Even higher dosages (120 mg every 4 h) have been evaluated. According to the prescribing information, this dosage was administered in four patients presenting significant hypotension half of them [25]. Of note, the landmark trial of Allen et al. [10] used a loading dose (0.7 mg/kg) followed by a weight-adjusted dosage (0.35 mg/kg) every 4 h for 21 days. In a patient with 80 kg, this dose would be 56 mg as a loading dose followed by 28 mg every 4 h, much lower than the recommended dosage, so this might suggest that the minimal effective dose of nimodipine in patients with aSAH remains to be determined.
Nimodipine-associated hypotension may lead to dosage splitting, dosage reduction, or therapy discontinuation [4, 5, 26, 27]. Several retrospective assessments of these practices have noted an association between modified nimodipine regimens and poor outcomes, but these analyses have a high risk for bias because nimodipine was often withheld on diagnosis of DCI or vasospasm and frequently along with the initiation of vasopressors for blood pressure augmentation [28,29,30]. Although this constitutes a common practice, splitting the dose might modify the pharmacokinetic saw-tooth profile of oral nimodipine and account for decreased efficacy, in contrast with the relatively constant plasma concentrations when using intravenous nimodipine.
In addition, there is huge variability in nimodipine concentrations in response to age, sex, renal and liver failure, and genetic polymorphisms [31]. Drug interactions must be considered, too, and, as previously noted, different nimodipine formulations and administration techniques may affect its bioavailability [7, 16, 31].
Although evidence suggesting that a correlation between nimodipine concentrations and patient outcomes is still scarce [31], the authors believe that future studies must be conducted to address whether there is such an association, and therefore a need for nimodipine dose individualization in patients with aSAH. In this direction, a study addressing cerebral nimodipine concentrations after oral, intravenous, and intraarterial administration is underway (NCT04649398) and might contribute to shed a light on the route and dosing of nimodipine in patients with aSAH. This would be especially interesting considering that most studies in this area include only patients with good-grade aSAH, and the requirements of nimodipine could be potentially different in patients with good-grade and poor-grade aSAH.
Timing and Duration
Oral or enteral nimodipine administration is usually recommended within 96 h of the bleeding, before the “vasospasm window” [7]. However, the optimal timing to start nimodipine is still debated [5], for example, the quality indicators of the Spanish Society of Intensive Care Medicine consider it a standard to use it as early as within 12 h of aSAH onset [32].
Additionally, it can also be debatable how many time should nimodipine be administered. Landmark studies [10, 11, 24] used the 21-day timeframe, as supported by the guidelines [5]. However, other authors suggest that treatment should not be longer than 14 days [7], which is, at least, reasonable, considering the classical timing of the high-risk window for angiographic cerebral vasospasm. Although there have been no prospective RCTs comparing different duration of treatment with oral or enteral nimodipine, retrospective single-center studies suggest that similar results can be obtained in 14 days [33, 34] or less [35], especially in patients with good-grade aSAH [34].
In the authors’ opinion, and considering the evolving knowledge in DCI pathophysiology and the growing concerns in the nimodipine safety profile, this constitutes an area for planning future trials.


留言 (0)