
記住我


Participants of this study were selected retrospectively from a cohort of first- and second-degree relatives of individuals with type 1 diabetes enrolled in the Type 1 Diabetes TrialNet Pathway to Prevention Trial (TNPTP) [21] at the TrialNet Clinical Center of the IRCCS Ospedale San Raffaele (OSR) from June 2012 to July 2019. TNPTP participants were screened for islet autoantibodies to glutamic acid decarboxylase (GADA), insulin (microinsulin antibody assay, mIAA), insulinoma-associated antigen 2 (IA-2A), zinc transporter 8 (ZnT8A) and islet cell antibodies (ICA). TNPTP participants who tested positive for autoantibodies in at least one of their previous visits were monitored with autoantibody testing, glycated hemoglobin (HbA1c), and a 2-h oral glucose tolerance test (OGTT) at 6-month intervals. Stage 1 was defined as the presence of ≥ 2 autoantibodies and normoglycemia (fasting glucose < 5.6 mmol/l and/or 2-h glucose < 7.8 mmol/l). Stage 2 was defined as the presence of ≥ 2 autoantibodies and dysglycemia (fasting glucose ≥ 5.6 mmol/l and/or 2-h glucose ≥ 7.8 mmol/l), while Stage 3 was defined as diabetes (fasting glucose ≥ 7.0 mmol/l and/or 2-h glucose ≥ 11.1 mmol/l). The complete TNPTP protocol is available online (http://www.clinicaltrials.gov/show/NCT00097292). The TNPTP study was approved by the OSR Ethics Committee (IRB# NHPROT32803-TN01). This project was performed using additional blood samples drawn during the visits for ancillary studies (IRB#TIGET004-DRI003).
Out of the 1316 relatives enrolled in the TNPTP cohort at OSR (OSR-TNPTP), 142 individuals were autoantibody-positive and underwent OGTT as per the TNPTP protocol. Inclusion criteria required the availability of glucose, insulin and C-peptide levels during a 2-h OGTT. Exclusion criteria comprised: (1) clinical manifestations of infection, such as fever, cough, or cold, within the two weeks preceding the study visit during which the OGTT was performed; and (2) concurrent treatments, encompassing antibiotics, immunosuppressive agents, or insulin therapy. Following these selection criteria, a total of 125 individuals were retrospectively chosen for inclusion in the current study. Each participant contributed data only once.
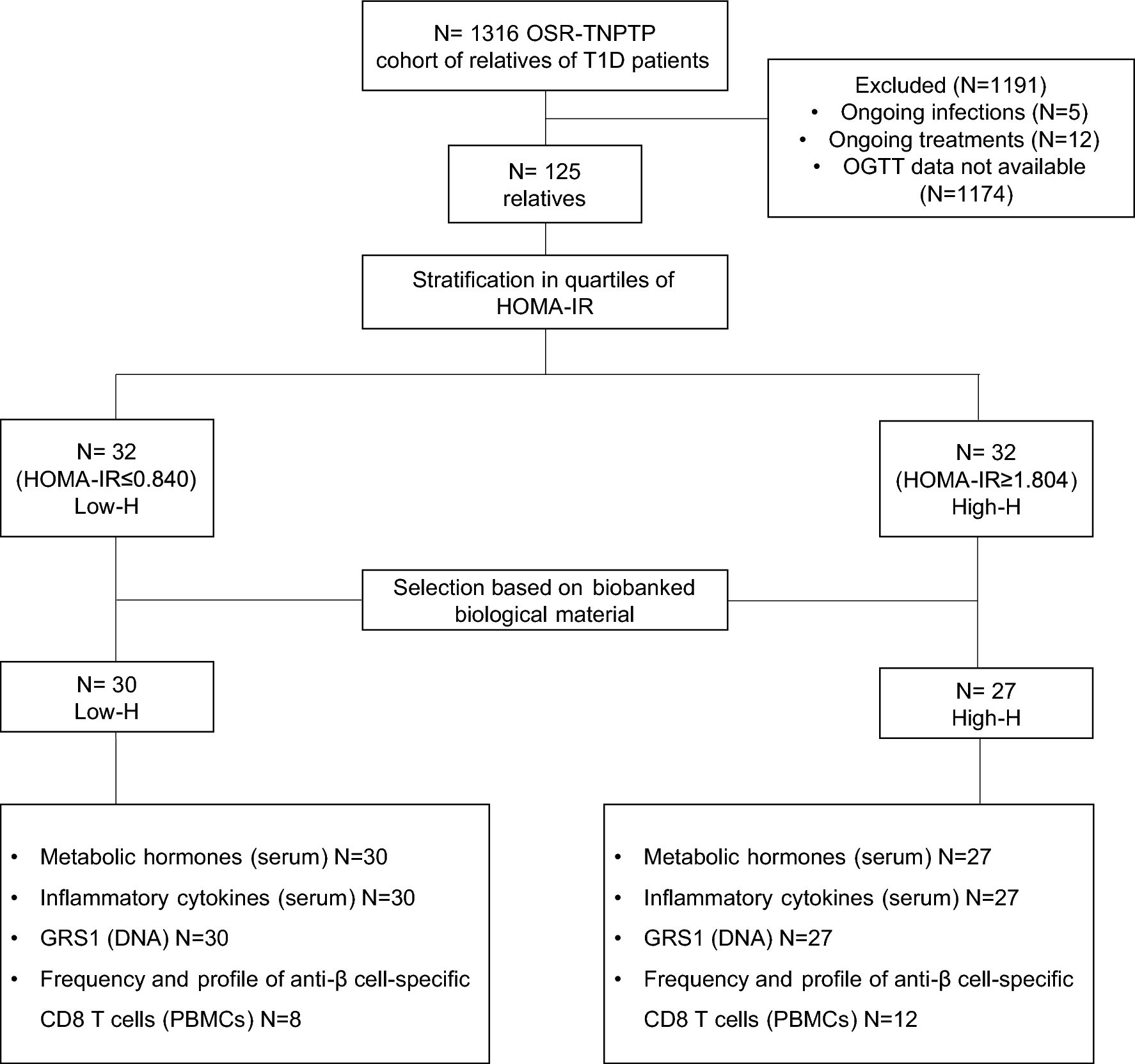
Selected individuals were then categorized into quartiles of insulin resistance, determined by Homeostatic Model Assessment of Insulin Resistance (HOMA-IR), with both the upper and lower quartiles included in the study. By specifically focusing on patients at the extremes of insulin resistance, our objective was to increase the probability of identifying potential metabolic, genetic and immunological disparities. Subsequently, an additional selection process was carried out based on the availability of biobanked biological samples (i.e., serum, whole blood, and peripheral blood mononuclear cells), collected during the same visit as the OGTT. The final cohort of chosen relatives consisted of n = 30 individuals for the low insulin resistance group (low-H) and n = 27 for the high insulin resistance group (high-H) (refer to Fig. 1 for the study design).
Fig. 1
Study design. 125 subjects were selected starting from a cohort of 1316 relatives of individuals with T1D, enrolled in the TrialNet Pathway to Prevention Trial (TNPTP) at the IRCCS Ospedale San Raffaele (OSR), based on the inclusion and exclusion criteria, including the availability of data from 2-h oral glucose tolerance test (OGTT). The Homeostatic Model Assessment of Insulin Resistance (HOMA-IR) was utilized as an indicator of insulin resistance to categorize relatives into quartiles. The lower and upper quartiles were identified, resulting in groups of 32 relatives with low insulin resistance (low-H) and 32 relatives with high insulin resistance (high-H), respectively. The groups were further reduced to 30 relatives for the low-H group and 27 for the high-H group based on the availability of biological materials. Various assays were conducted on this selected cohort, including the analysis of metabolic hormones and inflammatory cytokines in serum, the assessment of the T1D genetic risk score 1 (GRS1) using DNA, and the characterization of β-cell-specific CD8 T cells in peripheral blood mononuclear cells (PBMCs)
2-h Oral Glucose Tolerance Test (OGTT)Autoantibody-positive participants underwent an OGTT (oral glucose load dose 1.75 g/kg, maximum 75 g) after an overnight fast. C-peptide (ng/ml), glucose (mmol/l) and insulin (pmol/l) measurements were performed fasting and then after oral glucose intake at 30, 60, 90, and 120 min.
Metabolic indicesFor the metabolic characterization of our cohort, indices of insulin sensitivity and beta cell function were employed. Insulin resistance was calculated using the HOMA-IR [22]. The Matsuda index, which measures insulin sensitivity, is expressed by the ratio of 10,000 to the square root of the product between fasting glucose, fasting insulin, mean glucose and mean insulin during OGTTs [23]. Dysglycemia was defined as fasting glucose ≥ 5.6 mmol/l and/or 2-h glucose ≥ 7.8 mmol/l. The C-peptide area under the curve (AUC) was calculated using the trapezoidal rule, while the Insulinogenic Index (IGI) as the ratio of insulin (pmol/l) at 30 min minus fasting insulin (pmol/l) to glucose (mmol/l) at 30 min minus fasting glucose (mmol/l). Both are strong predictors of β-cell function [24, 25].
BMI percentile (BMIp) calculationBody mass index percentiles (BMIp) were determined based on sex- and age-specific charts from the Italian population (Italian.ref) of the childsds R package using R statistical Software (version 4.3.0).
Proinsulin/C-peptide ratioThe ratio between proinsulin (PI) and C-peptide has been used as a marker of endoplasmic reticulum stress in β-cells and predictor for β-cell dysfunction [26]. Quantification of proinsulin in the serum was determined by enzyme-linked immunosorbent assay (ELISA) (Human Total Proinsulin Elisa kit, EMD Millipore, Merck; cat# EZHPI-15 K, RRID: AB_3099413) and BioTek Epoch Microplate Spectrophotometer. C-peptide was measured with the Hormone Magnetic Bead Panel (EMD Millipore, Merck; cat # HMHEMAG-34 K) and Bio-plex MAGPIX Multiplex Reader (BIO-RAD).
Serum metabolic hormones and adipokinesThe gastric inhibitory polypeptide (GIP), leptin, pancreatic polypeptide (PP), active amylin and insulin (I) were measured in serum samples withdrawn after an overnight fasting using the Human Metabolic Hormone Magnetic Bead Panel (EMD Millipore, Merck; cat # HMHEMAG-34 K). Adiponectin, adipsin, resistin and plasminogen activator inhibitor-1 (PAI-1) were measured in the serum of fasting subjects with the Human Adipokine Magnetic Bead Panel (Millipore, Merck; cat # HADK1MAG-61 K). Measures were performed using the Bio-plex MAGPIX Multiplex Reader (BIO-RAD). The Bio-Plex Manager MP Software was used for data acquisition, quantification, and optimization of standard curves for metabolic hormones and adipokines; final concentrations are expressed in pg/mL.
DNA extraction and T1D genetic risk score 1DNA was extracted from whole blood samples using the Maxwell® RSC Instrument and the Maxwell® RSC Blood DNA Kit by Promega (cat #AS1400). The T1D genetic risk score 1 (GRS1), based on 30 SNPs associated with an increased risk of T1D [15], was calculated for each subject by summing the contribution of each allele as the product of the dosage and the natural logarithm of the odd ratio [27]. Four SNPs associated with the HLA class II risk haplotypes DR3 and DR4-DQ8 were analysed by droplet digital PCR (Bio-Rad, USA). All other risk SNPs were typed using the high-throughput OpenArray system (Life Technologies, USA) [28].
Inflammatory cytokinesGrowth related oncogene-alpha (GRO α), interferon-alpha2 (IFNα2), interferon gamma (IFNγ), interleukin 1 beta (IL-1β), interleukin 1 receptor antagonist (IL-1RA), interleukin 13 (IL-13), interleukin 15 (IL-15), interleukin 17-A (IL-17A), interleukin 6 (IL-6), interleukin 8 (IL-8), interleukin 10 (IL-10), interferon-gamma inducible protein 10 kDa (IP 10), monocyte chemoattractant protein 1 (MCP1), macrophage inflammatory protein-a alpha (MIP-1α), soluble CD40 ligand (sCD40L) and tumor necrosis factor alpha (TNFα) were measured in the serum samples using the Human Cytokine/Chemokine/Growth Factor Panel A Magnetic Bead Panel (EMD Millipore, Merck; cat# HCYTA-60 K) and the Bio-plex MAGPIX Multiplex Reader -BIO-RAD. Final concentrations are expressed in pg/mL.
PBMCs isolationAfter blood withdrawal, peripheral blood mononuclear cells (PBMCs) were isolated by density gradient centrifugation using Lympholyte® Cell Separation density gradient centrifugation media (Cedarlane, cat # CL5020) and frozen in Roswell Park Memorial Institute (RPMI) supplemented with dimethyl sulfoxide (DMSO) (10%) and fetal bovine serum (20%) for further experimentation.
Flow cytometry analysisFrom the cohort of 57 relatives selected for this study, 20 subjects—who tested positive for HLA-A2 (using PE anti-human HLA-A2 antibody, Biolegend, cat #343306, RRID: AB_1877228)—were selected to perform flow cytometry analysis for the study of islet-specific CD8 T cells. PBMCs were thawed and resuspended in fresh RPMI + 10% FBS (RPMI + 10% FBS + 1% glutamine + 1% P/S). First, cells were washed and stained for dead cell exclusion using BD Horizon™ Fixable Viability Stain 575 V (RRID: AB_2869702) at RT for 15 min in phosphate-buffered saline (PBS). Then, samples were washed and stained with insulin and GAD65-specific dextramers at RT for 10 min in FACS buffer (PBS + 1% bovine serum albumin + 0.1% sodium azide). Finally, cells were incubated using appropriate saturating concentrations of the following conjugated monoclonal antibodies; CD45 (RRID: AB_1236444), CD3 (RRID: AB_2744382), CD56 (RRID: AB_2916880), CD4 (RRID: AB_2870176), CD8 (RRID: AB_1645481), CD45RA (RRID: AB_2660984), CCR7 (RRID: AB_2033948), CD69 (RRID: AB_2561783), CD154 (RRID: AB_2743658), CD137 (RRID: AB_2871191) and LAG3 (RRID: AB_2869706), at RT for 20 min in FACS buffer. The list of anti-human monoclonal antibodies and anti-GAD65 and anti-insulin dextramers, including company, catalogue number, clone, peptide sequence (for dextramers) and concentration used, is provided in Supplementary Table 1 [29]. The FACSymphony™ A5 analyzer (BD Bioscience) was used for sample acquisition. Instrument performance was checked daily using CS&T Beads (BD Bioscience) and SPHERO Rainbow Beads (Spherotech Inc., Lake Forest, IL). Data acquisition and analyses were performed using FACSDiva v.8 (BD Pharmingen), and Flow-jo v.10 (Tree Star Inc.) respectively.
Statistical analysisTo ensure the representativeness of the population for genetic, metabolic, and immunological analyses, quartiles of the HOMA-IR index were calculated on the final OSR-TNPTP cohort consisting of 125 relatives. This decision was made as the International TNPTP cohort demonstrated significantly higher levels of HOMA-IR (OSR-TNPTP: mean 1.42, SD ± 0.80 vs. International TNPTP: mean 1.75, SD ± 1.57, p < 0.0001). The cohort of relatives of individuals with T1D was stratified based on quartiles, with Q1 = 0.840, Q2 or median = 1.320 and Q3 = 1.804. Subjects falling in the lower and upper quartiles were identified as the low insulin resistance group (low-H, HOMA-IR ≤ 0.840) and the high insulin resistance group (high-H, HOMA-IR ≥ 1.804), respectively. Data are summarised in tables as median and interquartile range (IQR) or as absolute number and percentage. Graphs are presented as median and interquartile range (IQR). Statistical analyses were performed with GraphPad Prism V.9.00 software (GraphPad). When comparing continuous variables of two independent groups, data were analysed using the Mann–Whitney test. In the case of comparison between multiple groups the Kruskal–Wallis test and Dunn’s multiple comparison test were used. Fisher’s exact test was used for comparison between nominal variables. To test the correlation among continuous parameters, the Spearman’s rank-order correlation analysis was performed. To determine the effect of BMIp on relationships between variables of interest and HOMA-IR, two linear models were constructed using R (version 4.3). In the first model, each variable of interest was modeled solely as a function of the HOMA-IR group variable. In the second model, each variable was considered a dependent variable, with BMIp and HOMA-IR group as independent variables. Missing BMIp values were removed prior to analysis to avoid bias. Data are considered statistically different when p value was < 0.05; *graphically indicates p < 0.05, **graphically indicates p < 0.01, ***graphically indicates p < 0.001, ****graphically indicates p < 0.0001.
留言 (0)