
記住我
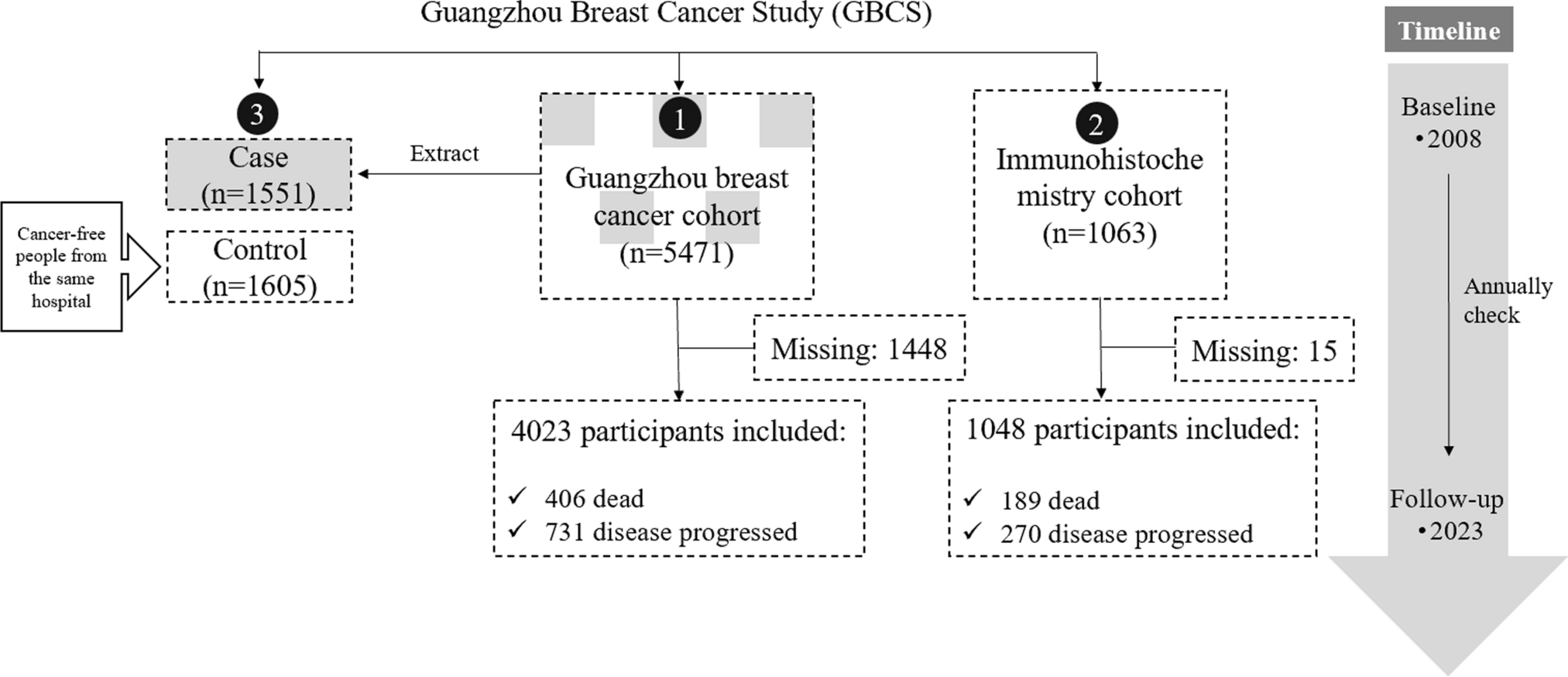




Between 1993 and 1997, 160,727 men and women were invited to participate in the Danish prospective cohort study “Diet, Cancer and Health (DCH)” in which 57,053 participants were included [15]. To be eligible for inclusion, participants had to be born in Denmark, live in the Copenhagen or Aarhus areas and with no previous cancer diagnosis registered in the Danish Cancer Registry. At enrolment, all participants filled in self-administered questionnaires about their diet and various lifestyle factors and attended a physical examination at one of two study centers located in Copenhagen and Aarhus where their anthropometrics were measured. Further details about the study can be found elsewhere [15]. For the estimation of alcohol consumption trajectories, we excluded all male participants (n = 27,178), women with a cancer diagnosis at baseline (n = 538), missing follow-up information (n < 5) and women without baseline information (n = 33) (Fig. 1). Furthermore, women with an energy ratio in the top or bottom 1% of the energy intake to calculated energy requirement distribution were excluded (n = 583). Thus, we used information from 28,720 women to estimate alcohol consumption trajectories. For the proportional hazard regression model, we further excluded women who were premenopausal at baseline (n = 2,077) and women with missing information on covariates considered potential confounding variables which include: physical activity level, smoking status, educational level, BMI, age at first full term pregnancy, age at menarche, breast feeding, and ever use hormonal replacement therapy (n = 2,100). In total, we included 24,543 women in the regression model (Fig. 1).
Fig. 1
Flow of participants into the study1
1Note: LCMM: latent class mixed model; n: number; EI/ER ratio: energy intake to energy requirement ratio
Alcohol consumptionAll participants completed a validated 192-item food frequency questionnaire (FFQ), on which they reported their average intake of food and beverages including alcohol over the last 12 months [15, 16]. Using a lifestyle questionnaire, the participants were also asked to retrospectively report their average intakes of alcohol at four periods of their lives (at the ages of 20, 30, 40, 50 years) to reflect lifetime intakes of alcohol. See Supplementary Table 1 for the number of women with available information about their alcohol intake at the different ages. The participants reported their intake in 12 categories ranging from “never” to ≥ 8 times per day. In terms of their alcohol consumption, the participants reported their average frequency of consumption of beer (3 types, in bottles of 330 ml), wine in standard glassed (125 ml), fortified wine used for drinks (glassed of 60 ml) and spirits used for drinks (30 ml) [15, 17]. The amount of alcohol (measured as ethanol) in each beverage varied according to beverage type: light beer: 8.9 g/bottle; regular beer: 12.2 g/bottle; strong beer: 17.5 g/bottle; wine: 12.5 g/glass and fortified wine: 9.3 g/drink; spirits: 9.9 g/drink [17].
Ascertainment of menopausal status and first primary malignant female breast cancerIn this study, we focused only on incident BC among women who were postmenopausal as the number of BC cases among women pre-menopausal was considered too low to provide sufficient statistical power (n = 134 after exclusion of women with incomplete data on potential confounders). Menopausal status was determined at baseline and according to various information about the women’s menstrual history as described previously [18]. Women were categorised as postmenopausal if they had no periods of menses during the preceding 12 months from baseline or had undergone surgically induced menopause due to a bilateral ovariectomy. Women with no information about their menstruation history, women who reported having undergone a hysterectomy surgery or exogenous hormones use were characterised as postmenopausal if they were ≥55 years. Women were categorised as perimenopausal if they had <9 menstrual periods the preceding year or if they had had menstruation the preceding year, but not at the time of the baseline assessment. Women aged 46–55 years old were categorised as perimenopausal if information about their menstruation history was missing or they stated exogenous hormone use or having undergone a hysterectomy. In the current study, we considered perimenopausal women as being post-menopausal (n = 4,114 women after exclusion of women with incomplete data on potential confounders) as we assumed that these women would have reached menopause at the time of diagnosis or end of follow-up. Cases of first primary malignant BC were identified through record linkage to the Danish Cancer Registry using each participant’s unique personal identification number. First primary malignant female BC (C50) was defined according to the International Classification of Disease for Oncology.
Covariate assessmentFrom the lifestyle questionnaire administrated at baseline (between 1993 and 1997), we obtained information about several lifestyle and reproductive factors which included educational level (considered a proxy for socioeconomic status), smoking status and physical activity level, age at birth of first child, age at menarche, breast-feeding history, and use of hormonal replacement therapy. The participants’ height and weight were measured by trained lab technicians. The participants’ height was measured while standing without shoes and to the nearest 0.5 cm while the participants’ weight was measured in light underwear using a digital scale to the nearest 0.1 kg. BMI was calculated as weight (kg) divided by height squared (m2) [15].
Statistical analysisTo associate trajectories of alcohol consumption with the risk of BC, we adopted a multi-step analysis approach [19, 20]. First, we identified subgroups of women with distinct alcohol consumption patterns across adulthood using LCMM. Second, we used a proportional hazard model to investigate the association between the identified latent classes and risk of first primary malignant BC.
Analysis step 1: trajectory estimationWe fitted LCMM from all available alcohol measurements (measured at baseline and at the ages 20,30,40 and 50 years) irrespectively of the participants’ menopausal status and available covariate information. All measurements of the participants’ alcohol intakes were log-transformed (log(x + 1)) to account for their non-normal distribution. We modelled the trajectories as a function of participants’ age (rescaled and recentred: (age-35/13)) assuming a quadratic time trend both at the population level and at the individual level with random effects to account for the intra-individual correlation between the alcohol measurements of the same woman. We used a quadratic time function determined based on visual inspection of 100 randomly selected women’s individual trajectories of alcohol consumption. The LCMM models were estimated within the maximum likelihood framework for a varying number of latent classes ranging from 1 to 6. To prevent convergence towards a local suboptimal maximum and to fully explore the parameter space, we ran the estimation procedure from 100 vectors of random initial parameter values based on the model parameters of the 1-class trajectory model. Furthermore, for the 5 and 6-class models, respectively, we manually specified initial values based on the model parameters obtained from models with a lower number of latent classes. We determined the most appropriate number of latent classes according to several statistical criteria: the Bayesian Information Criteria (BIC), entropy, the Integrated Classification Likelihood Criterion (ICL) and the posterior probability classification [19, 21]. Furthermore, we did not retain latent classes considered too small (<5% of the participants) as the number of BC cases within each class would be too limited for further analysis (see the supplementary method for a detailed description of the criteria). To further evaluate the goodness-of-fit of the selected model, we plotted the weighted-subject specific predicted trajectories against the weighted mean observed trajectories. After determination of the final latent class model, each woman was assigned to the trajectory class to which they had the highest posterior probability of belonging given their measures of alcohol intakes for the purpose of using standard summary statistics to describe baseline socio-demographic, lifestyle, and reproductive characteristics of the women according to the assigned latent class. We used the “GRoLTS-Checklist: Guidelines for Reporting on Latent Trajectory Studies” to guide our trajectory estimation [22].
Analysis step 2: risk of breast cancer according to the estimated alcohol trajectory profilesTo investigate the association between the latent class structure and the risk of BC, we estimated class-specific hazard ratios (HR) and corresponding 95% confidence intervals (CI) using a parametric proportional hazard model assuming proportional hazards across latent classes. The time to diagnosis of first primary malignant BC was right censored by death, emigration, or loss to follow-up, which ever came first. We maximized the joint likelihood by keeping the parameters of the LCMM fixed while estimating the parameters of the hazard model. This allowed us to model the risk of BC according to the true latent class structure while properly accounting for the inherent classification error in the posterior assignment [19]. We fitted two parametric survival models with proportional hazards across classes. One model assuming a Weibull baseline hazard function and a second model approximating the baseline hazard by a cubic M-splines with 5 and 4 knots, respectively and compared the models according to the AIC. According to the AIC, we selected the more flexible hazard specific model with cubic M-splines with 4 knots and modelled the instantaneous risk of BC according to participant age. The estimated procedure accounted for delayed entry. We used two levels of adjustment for potential confounding factors. In Model 1, we adjusted for participant age (underlying timescale) and baseline date of recruitment into the cohort (in quintiles). In Model 2, we further adjusted for the following lifestyle and reproductive factors: physical activity level (inactive, moderately inactive, moderately active, active), smoking status (current smoker, former smoker, never smoker), educational level (primary, technical/professional school, secondary school, higher education), BMI (<18.5 kg/m2, 18.5–24.9 kg/m2, 25-<30 kg/m2, ≥ 30 kg/m2), age at first full term pregnancy (no full-term pregnancy, ≤ 21, 21–30, >30 years), age at menarche (≤12, 12–14, >14 years), breast feeding (yes, no), and ever use hormonal replacement therapy (yes, no). Potential confounding variables were selected a priori based on previous literature and a directed acyclic graph (Supplementary Fig. 2). The directed acyclic graph was created using the online resource “DAGitty” [23].
We performed all statistical analyses in R version 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria), primarily using the lcmm R package, (Version 2.1.0) [24]. We used the “hlme” function for analysis step 1 and the “externVar” function for analysis step 2.
留言 (0)