
記住我




The EPIC study is a large multicenter cohort study including 521,323 participants enrolled between 1992 and 2000 in 23 centers across 10 European countries. EPIC aims to investigate the relationship between nutrition and lifestyle with cancer. At baseline, data on dietary and non-dietary variables, anthropometric measurements, and blood samples were collected from participants residing in the surrounding area of the given study center. Written informed consent was obtained from each participant, and the EPIC study was ethically approved by IARC and the respective centers [16, 17].
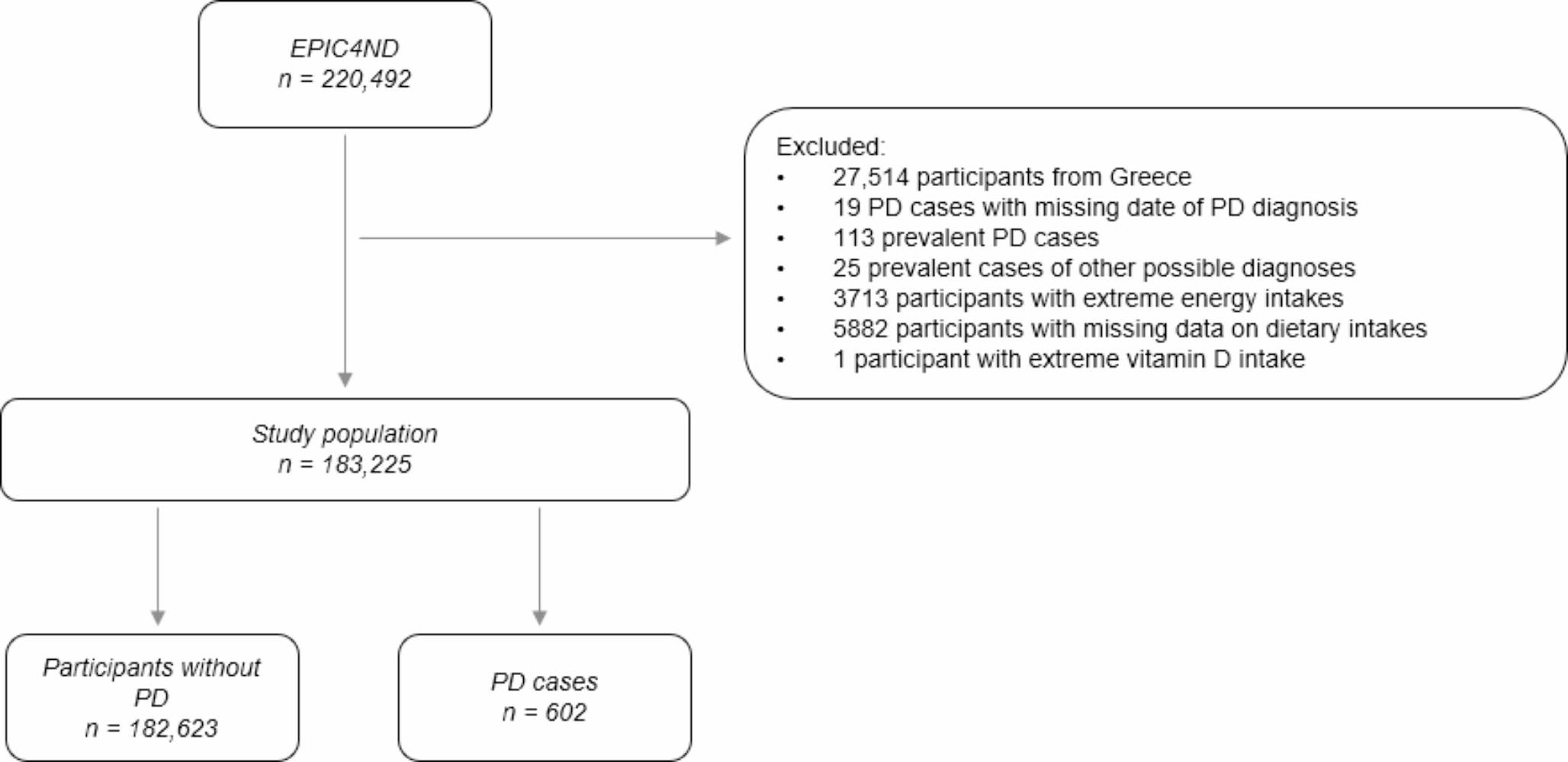
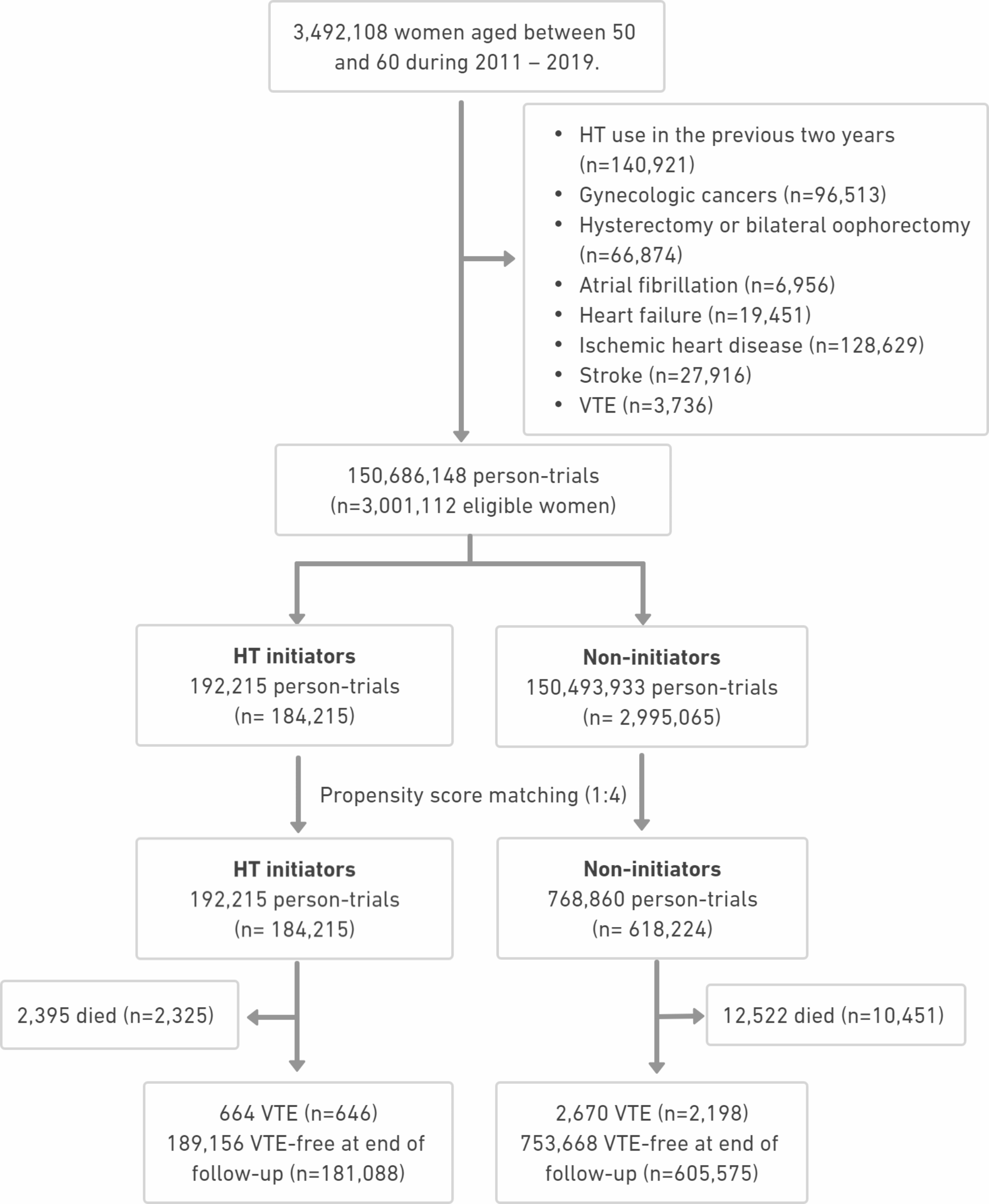
EPIC4NDThe EPIC4ND cohort, which is nested within the EPIC cohort, aims to investigate the association between pre-diagnostic risk factors and the development of PD, amongst other neurodegenerative disorders. It comprises data from 220,492 subjects in 13 of the 23 EPIC centers across 7 out of 10 European EPIC countries. For the present study, we used data from 183,225 subjects recruited in Sweden (Umeå, Malmö), the UK (Cambridge), the Netherlands (Utrecht), Germany (Heidelberg), Spain (Navarra, San Sebastian, Murcia) and Italy (Turin, Varese, Florence, Naples). The Naples and Utrecht cohorts only include women contrary to the remaining centers [17]. Figure 1 depicts a flowchart of the inclusion criteria for the study population. 27,514 participants from Greece were excluded due to GDPR issues. Furthermore, 19 PD cases with a missing date of diagnosis, 113 prevalent PD cases, defined as having received a diagnosis of PD before the date of recruitment or the same day, and 25 prevalent cases of other possible diagnoses, identified after case ascertainment and distinct to Parkinson´s disease, were also excluded. 3713 participants whose energy intake/energy requirement ratios fell outside the top or bottom 1% of all participants were excluded, alongside 5882 participants with missing data on dietary intakes. In addition, one participant exhibiting a vitamin D intake twice as high as the second highest intake level was also excluded due to implausibility.
Fig. 1
Flowchart of cohort participants included in the analysis
Dietary intake assessmentsData on dietary intake was assessed at baseline using different dietary assessment methods across countries and centers. In Italy, the UK, the Netherlands, Sweden and Germany extensive (semi-quantitative) food-frequency questionnaires (FFQs) were used to estimate individual average portion size. Questionnaires were self-administered, except for Naples in Italy, were face-to-face semi-quantitative FFQs were conducted. In Spain, face-to-face diet history questionnaires, structured by meals, were administered. In Malmö, in addition to the FFQ, data was collected through a 7-day record on hot meals [18].
To address the issue of limited comparability due to different dietary assessment methods, additional data on dietary intake was obtained through a computer-assisted 24-hour dietary recall (24-HDR) in representative sub-samples. These sub-samples encompassed 5–12% of study participants in each sub-cohort, except for the UK (1.5%). Data from the 24-HDR served as a reference method to address systematic over- or underestimation between centers in the initial dietary assessments [19].
Values for daily energy intake, calcium and vitamin D intakes were computed based on country-specific food composition tables, which were harmonized across the countries participating in EPIC (EPIC Nutrient DataBase, ENDB) [20].
Non-dietary variablesInformation on lifestyle, menstrual and reproductive history, and past medical history was collected through questions on education, socio-economic status, and occupation; history of previous illness, disorders or surgical operations; lifetime history of tobacco use; lifetime history of alcohol consumption; physical activity; menstrual and reproductive history; and utilization of hormones for contraception and postmenopausal replacement therapy. Height, weight, and waist and hip circumference were measured on all subjects in all centers at baseline, except for Umeå where only weight and height were measured [16].
Outcome assessmentFor ascertainment of PD cases, an EPIC4ND template for clinical data collection was developed upon which a possible final diagnosis was made. These included PD, multiple system atrophy, progressive supranuclear palsy, vascular parkinsonism, dementia with Lewy bodies, essential tremor, PD with essential tremor and unclassifiable parkinsonism, amongst others. Depending on the amount and quality of available data (“poor”, “good” or “excellent”) as well as the extent of confidence of the neurologist expert (“low”, “medium” and “high”), each diagnosis was thereafter labelled with an EPIC4ND label (“definite”, “very likely”, “probable” or “possible”). Subsequently, ascertainment consisted of two phases: In phase I, potential cases were identified via record linkage with at least one local source of information to minimize the chances of false negatives. Resources for record linkage encompass hospital discharge registries, drug databases, mortality records, questionnaires, amongst others. In phase II, said potential cases were re-reviewed by specialists in movement disorders and a final diagnosis was established according to the standardized protocol described above and previously [17].
Statistical analysisDescriptive statistics were calculated separately for participants that remained without PD diagnosis during follow-up, and for incident PD patients, with median and interquartile range for continuous variables, and proportions for categorical variables. Crude, basic- (sex-, age- and country-adjusted) and multivariable-adjusted hazard ratios (HRs) and their 95% Confidence Intervals (CIs) were estimated from the Cox proportional hazards model with age as the underlying time scale for each exposure of interest: total dairy, milk, yogurt, cheese, calcium and vitamin D intake. Dietary exposure variables under study were classified into sex-specific quartiles based on the distribution of intake observed among non-cases. Separate models were fit for each exposure of interest, using the lowest quartile as the reference category. P for trend was calculated by entering the quartile indicator variable into the models as a continuous variable. Additionally, HRs and 95% CIs were estimated from Cox proportional hazards model for every additional 100 g/d consumption of milk separately by fat content (skimmed, semi-skimmed and whole milk).
Male gender, age, smoking and coffee consumption are widely acknowledged as factors related to PD risk [1, 6, 7] and they may influence dietary and dairy consumption habits. Therefore, the multivariable-adjusted analysis was adjusted for these factors. Furthermore, we included previously established confounders into the multivariable-adjusted model, such as BMI, highest level of school education, physical activity, alcohol consumption and diabetes status. Since this study aims to investigate the risk of PD in association with dietary factors, we further adjusted for energy intake. Additionally, adjustment was made for country due to differences in data collection methods across study centers and variations in dietary habits across EPIC countries. In conclusion, the main model was adjusted for sex, age at recruitment, country of residence, BMI, highest education level (none, primary school completed, technical/professional school, secondary school, longer education, or not specified), physical activity (inactive, moderately inactive, moderately active, active, or not specified), smoking history (never, current (1–15 cig/day), current (16–25 cig/day), current (26 + cig/day), former (quit ≤ 10 years), former (quit 11–20 years), former (quit 20 + years), current (pipe/cigar/occas), or not specified), alcohol consumption, coffee consumption, diabetes status (no, yes, or not specified) and energy intake. BMI (kg/m2), alcohol consumption (g/day), coffee consumption (ml/day) and energy intake (kcal/d) were included in the model as continuous variables. To account for proportional hazards, we adjusted for age in 5-year steps and stratified the analysis by country. In a supplementary analysis, we investigated the associations of the individual covariates with PD risk.
Furthermore, we conducted sensitivity analyses by excluding the first 5 years of follow-up to reduce potential reverse causation bias. In a second sensitivity analysis, we only included cases with a PD diagnosis that had previously been labelled as “definite” or “very likely” (n = 314).
Since female gender and smoking confer as potential protective factors for PD, and conflicting evidence concerning the influence of overweight exists, we evaluated potential effect modification by running the analyses stratified by sex, by smoking status (never and ever smokers) and by BMI (BMI < 25 and BMI ≥ 25). Due to differences in dietary assessment methods across country, we conducted separate analyses for each country. For the latter, we modelled the dietary variables continuously, as there were too few cases for subgroup analysis by quartiles. Statistical heterogeneity between subgroups was assessed using interaction terms and the Wald statistic.
Additionally, we investigated the association of calcium and vitamin D with PD risk by food sources (from dairy products and from other food sources) overall, in men and in women. Consumption of calcium and vitamin D from other sources was computed by calculating calciumtotal – calciumdairy or vitamin Dtotal – vitamin Ddairy. Sex-specific quartiles were calculated individually for calcium intake from dairy, calcium intake from other sources, vitamin D intake from dairy and vitamin D intake from other sources among non-PD-diseased participants.
Statistical significance was set at the α = 0.05 level. The data analysis for this paper was generated using R software version 4.3.1 [21], and SAS software, Version 9.4. Copyright © 2024 SAS Institute Inc. SAS and all other SAS Institute Inc. product or service names are registered trademarks or trademarks of SAS Institute Inc., Cary, NC, USA.
留言 (0)