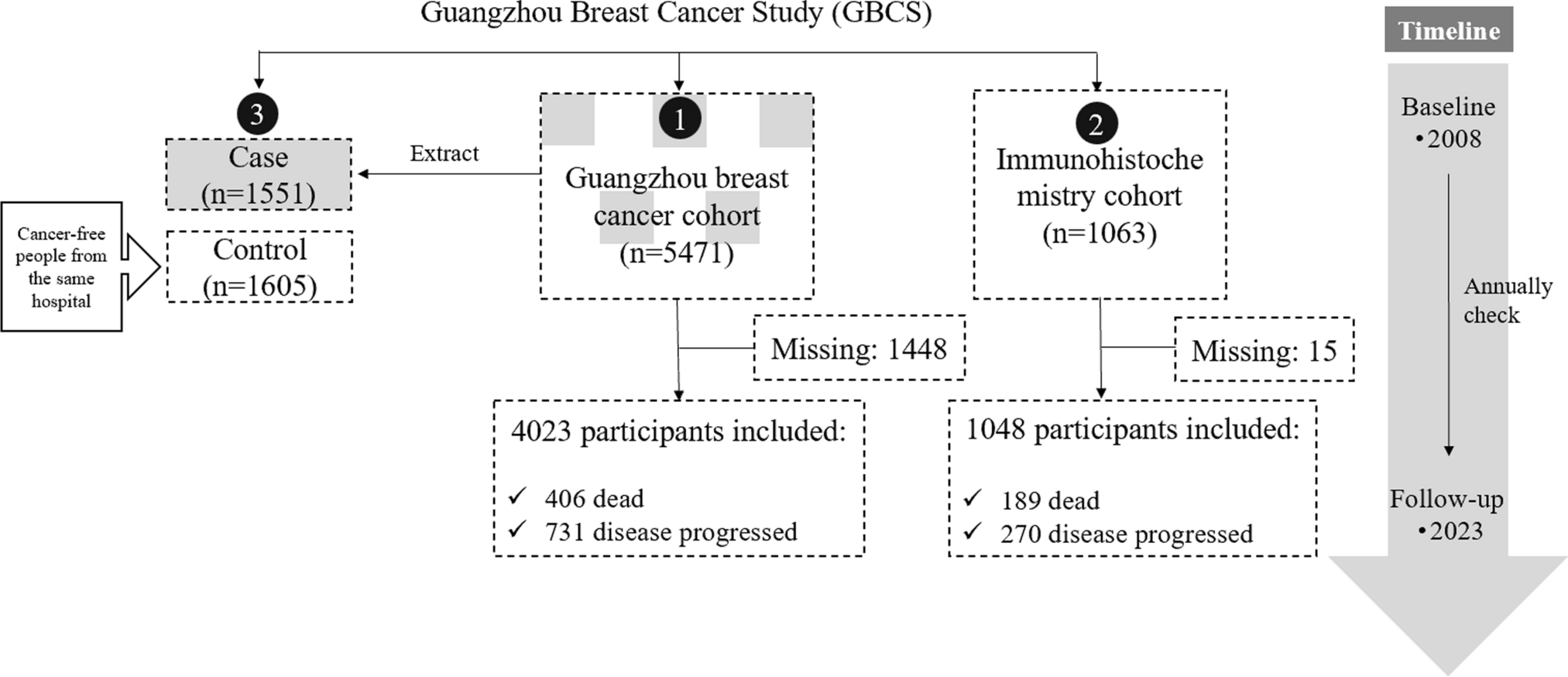
The GBCS consists of three interrelated studies: a Guangzhou breast cancer cohort, a case–control study, and an immunohistochemistry (IHC) cohort, each designed to investigate different aspects of BC in South China.
Guangzhou breast cancer cohort
The Guangzhou breast cancer cohort is a patient-based, prospective cohort study designed to explore the risk factors and prognosis of BC in South China. Participants were recruited from the First Affiliated Hospital, Second Affiliated Hospital and Cancer Center of Sun Yat-sen University from October 2008 to January 2018. Initially, 9029 patients with various breast diseases were enrolled in the study, all of whom provided informed consent (Supplementary Table 1). Among these participants, 5471 were confirmed to have BC and met the inclusion criteria for the Guangzhou breast cancer cohort, which included: (a) a pathological diagnosis of primary BC; (b) newly diagnosed cases; and (c) residency in the Pearl River Delta region for at least five years. Exclusion criteria were applied to exclude patients with a history of malignancy or mental illness, those unable to communicate due to severe illness, and those with cognitive impairments. Of these 5471 BC patients, 335 were diagnosed with ductal carcinoma in situ and 5136 had invasive BC.
Case–control study
In the GBCS case–control study focuses on identifying risk factors for the occurrence of BC. From October 2008 to March 2012, 1736 women diagnosed with BC from Guangzhou breast cancer cohort (as mentioned above) were unselectively included as cases. Moreover, cancer-free controls, frequency-matched by age, were selected from women undergoing routine medical examinations at the same hospitals during the same period. The inclusion criteria for controls included the absence of breast malignancy, confirmed by mammography, B-ultrasonography or self-reported, and residency in the Pearl River Delta region for at least 5 years. After excluding individuals diagnosed with other cancers, those with mental illness, and those who declined to complete questionnaires or donate blood samples, the final study included 1551 cases (89.3% participation rate) and 1605 controls (90.5% participation rate).
Immunohistochemistry (IHC) cohort
The GBCS IHC cohort investigates the underlying mechanisms of BC progression. This cohort includes 1063 women diagnosed with primary invasive BC, with tumors larger than 1 cm, recruited from the Cancer Center of Sun Yat-sen University between January 2008 and December 2015. Exclusion criteria included a history of other malignant tumors or mental illnesses (such as Alzheimer’s disease) and severe illnesses or language difficulties that prevent completion of the questionnaire. Histone modification markers and protein levels in tumor and adjacent tissues were assessed using tissue microarrays (TMAs) and immunohistochemistry.
How is the cohort followed up?
The GBCS cohort employs both active and passive follow-up methods. Active follow-ups are conducted every three months during the first year after diagnosis, either via phone calls or outpatient visits. In the second and the third years, follow-up occur every six months. Thereafter, participants are followed up annually until death. These follow-ups collect vital information, including survival statuses, treatment details, disease history, occupational history, post-diagnostic lifestyle changes, and updated contact details. Detailed follow-up variables are shown in Table 1. Passive follow-up is conducted through the hospital’s electronic medical record system, which provide authoritative data on disease progression and mortality. This method enables the capture of comprehensive clinical information, such as serum tumor markers, cell types and lipid profile, which are meticulously retrieved from medical records. As of 31 December 2023, at least four rounds of follow-up have been completed for all patients, with 4023 (73.5%) participants of Guangzhou breast cancer cohort and 1048 (98.6%) participants of IHC cohort being successfully followed up.
Table 1 Summary of follow-up variables in the Guangzhou Breast Cancer Study (GBCS) cohortWhat has been measured?
The GBCS collected a comprehensive range of data through structured questionnaires, clinical records and laboratory assays to investigate BC etiology, progression and outcomes. All GBCS participants completed a structured questionnaire developed by the Breast Cancer Epidemiology Research Group of Vanderbilt University, tailored to reflect current research on BC etiology and the demographic characteristics specific to the Guangdong region. Baseline data were obtained by face-to-face interviews, typically lasting 30–60 min [10,11,12], and included information on demographic factors, menstrual and reproductive history, disease history, contraceptive use, hormone therapy, dietary history, physical activity, occupational history, personal habits, and family history of cancer. Detailed baseline characteristics of the participants from the questionnaire are shown in Table 2. Furthermore, clinical data, such as tumor size, nodal status, clinical stage, and receptors status (i.e., estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2)), were meticulously retrieved from medical records. Participants fasted for 10–12 h before providing blood and urine samples, which were collected under the supervision of trained research assistants and stored at − 80 °C until further analysis. Each participant was assigned a unique identity number to ensure the accuracy and traceability of the samples.
Table 2 Summary of questionnaire data collected at baseline in the Guangzhou breast cancer cohort, IHC cohort, and case–control studyA wide range of laboratory variables was measured, including 26 urinary metals, 53 single nucleotide polymorphisms (SNPs), 27 cytokines, 14 histone modification markers, 16 proteins, 4 Epstein-Barr virus (EBV) antibodies, anti-Toxoplasma gondii (T. gondii) and anti-Chlamydia trachomatis (C. trachomatis) IgG. Each laboratory variable and the corresponding measurement sample are shown in Table 3.
Table 3 Summary of laboratory variables measured in the Guangzhou breast cancer cohort, IHC cohort, and case–control studyThe study was in accordance with the Declaration of Helsinki and approved by the Sun Yat-sen University Ethics Committee (Institutional Review Board approval number: 2012–8).
Urine metal detection
Twenty-six metals were quantified using inductively coupled plasma mass spectrometry (ICP-MS) (Agilent 7500ce ICP-MS, Agilent Technologies). Before analysis, urine samples were diluted with dilute nitric acid. The quantification of metals was performed by ICP-MS, calibrated with external standards provided by Spex Industries, with internal standards (89Y, 103Rh and 175Lu) added to each sample to ensure accuracy [13]. Samples underwent at least three replicate analyses, with rigorous quality control, including matrix blanks and quality-control samples, to avoid cross-contamination and ensure precision.
DNA isolation and genotyping
Genomic DNA was extracted from blood samples using the TIANamp Genomic DNA Kit (TianGen Biotech Co., Ltd., Beijing, China). Fifty-three SNPs were genotyped using Sequenom’s MassARRAY system (San Diego, California, USA) [14, 15]. Both positive and negative control methods were used for quality control, with 5% of samples being randomly selected for duplicate testing, achieving a 100% concordance rate.
Construction of tissue microarray (TMA) and IHC
Histone modification markers and protein levels were evaluated using TMAs and IHC [16]. TMAs were proceed through a series of steps, including antigen retrieval, blocking and incubating with specific antibodies. IHC stained sections were then digitally captured using the Pannoramic Scanner and analyzed with CaseViewer software. Staining intensity (scored from 0 to 3) and the percentage of positive strained tumor cells (0%–100%) were evaluated by an experienced pathologist blinded to the clinical data.
Serological tests
Serum cytokine levels were quantified using the Bio-Plex Pro Human Cytokine 27-plex assay (Bio-Rad, M500KCAF0Y) on a Luminex 200 platform (Luminex Corporation, Austin, TX, USA), allowing for rapid and accurate multiplex detection.
IgA and IgG antibodies against EBV VCA-p18 and EBNA-1 were measured using enzyme-linked immunosorbent assay (ELISA) kits (Zhongshan Bio-Tech, Zhongshan, China) [17]. The assays were standardized using a reference serum provided with each kit, with defined optical density (OD) cut-off values determining seropositivity [18].
Anti-T. gondii IgG was measured using commercial ELISA kits (Haitai Biological Pharmaceuticals Co., Ltd, Zhuhai, China) [19], with results validated against positive, negative, and critical controls. Similarly, anti-C. trachomatis IgG and total IgG were detected using ELISA kits (Savyon diagnostics, Israel and Cusabio Biotech Co, China, respectively), with seropositivity defined as a cut-off index (COI) higher than 1.1. All serological assays were conducted according to the manufacturer’s instructions, with blinded assessment to prevent bias in the analysis of case–control differences.








留言 (0)