The management of CH, one of the most painful and disabling forms of headache, has shifted with the development of new medications like galcanezumab, even as a first line of treatment [6, 13,14,15]. To the best of our knowledge, this is the first report with galcanezumab in Brazilian CH patients showing the effectiveness, tolerability, and pragmatic approach position from headache specialists for this primary headache.
Efficacy of galcanezumab in cluster headache
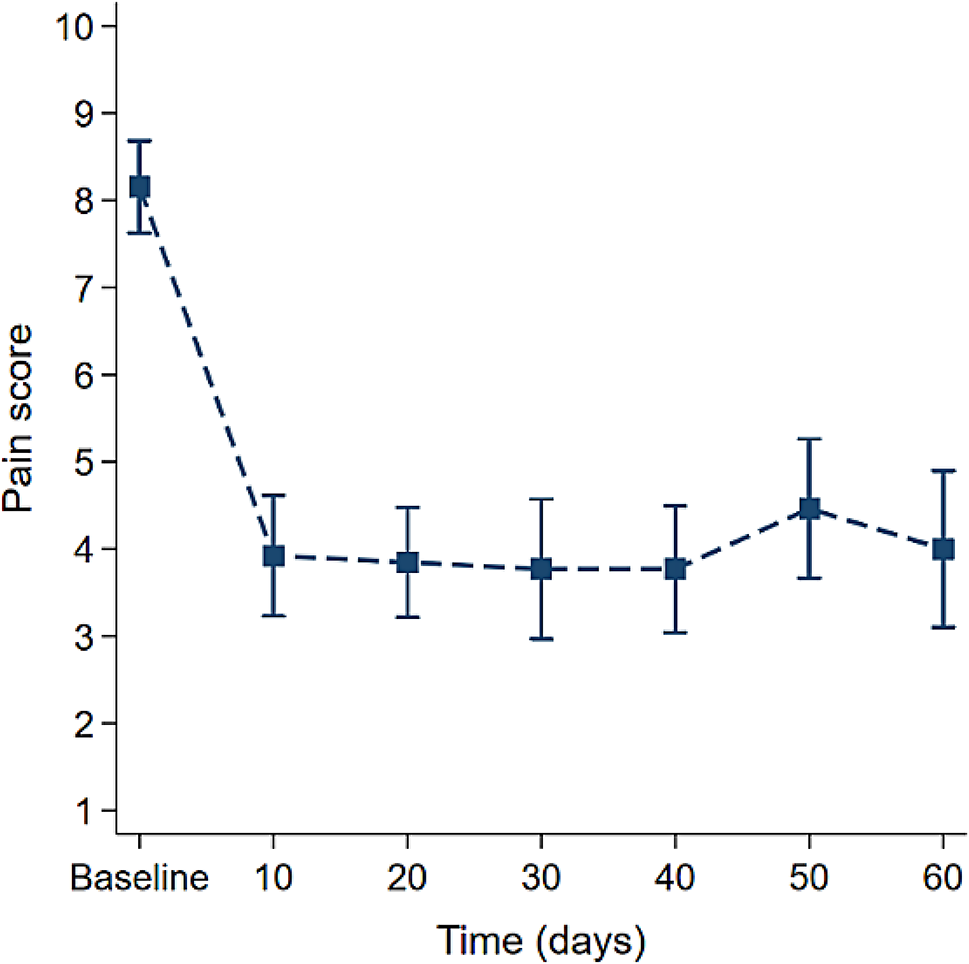
The outcomes of the present study bring to light a significant decrease in the number of headache attacks, with 64.8% of the patients with eCH achieving a ≥ 50% decrease in the number of attacks within three weeks of its subcutaneous administration. They are consistent with prior research [13, 14] for the preventive treatment of eCH. Although we do not know whether some patients improved due to a spontaneous remission, our timeframe to evaluate headache frequency reduction was, as previously reported in studies [14], three weeks. However, it is noteworthy that chronic sufferers also revealed at least some degree of reduction in headache severity (42.8% of the cCH patients and 50% of those cCH who were not lost to follow up). These results are even more important since the typical first-line medication verapamil may require an uncomfortable posology (three times a day), and promote tolerability issues such as constipation and AV conduction abnormalities [4, 5].
In our study, 66% of patients had a reduction in headache attacks ≥ 50% after 3 weeks with 300 mg doses of galcanezumab. Other studies that also evaluated the efficacy of galcanezumab in eCH in real-world patients found similar results, but used a dose of 240 mg galcanezumab [16,17,18].
Galcanezumab is a monoclonal antibody that targets CGRP and has been shown to be an effective treatment in stopping CH attacks. CGRP is found throughout the trigeminovascular system and is elevated in the jugular blood and tear fluid of patients with CH, both interictally and during attacks [19]. There is no doubt that CGRP plays an important role in the pathophysiology of CH, as CGRP infusion induces headache attacks in CH patients by promoting activation of the trigeminal-autonomic reflex [20] and its reduction with symptomatic treatment produces improvement [8,9,10].
Expert preferences and future directions
The panel of experts formed within the framework of this study also points out the need to tailor treatment for CH depending on whether CH is manifesting for the first time, the frequency and severity of the attacks, the patient’s particular conditions as the current time of bout duration and response to the previous therapy. It also describes the priority order for choosing treatment options, the likelihood of combining approaches, the place for new therapeutic agents, such as galcanezumab, and the consulting profile for the follow-up visits. Interestingly, for the whole panel of experts, galcanezumab was a treatment option to start even for chronic patients, despite its demonstrated lack of efficacy [13]. It also emphasized that non-cluster headache treatments, such as onabotulinumtoxinA, did not yet grab Brazilian paradigms of treatment for CH, despite existing questionable evidence [21].
The next steps in the assessment of galcanezumab should aim at developing more studies, especially for the heretofore understudied populations such as younger, older, and patients with cCH. Moreover, the development of further studies on the efficacy of combining galcanezumab with other traditional or novel treatments such as neuromodulation will be useful and are warranted in improving CH management.
Based on the data from the 10 Brazilian experts on the treatment of cluster headaches, which was not meant to represent the country guidelines, bring forward the following expert preferences consensus (Table 5):
Table 5 Expert consensus on the treatment of cluster headachesLimitations and strengths of the study
The current study offers accountabilities of real-world experience of CH using galcanezumab with the following limitations. First, a limitation is the uncontrolled design, although the patients were consecutive. Second, bias in treatment selection was limited by the discussion of each subject between 5 experts to decide the evaluation and treatment. Third, we had a 15.9% attrition rate, which may have been related to drug effectiveness, adverse effects, or cost issues since Brazilians rarely receive it from insurance or medical plans and have to purchase the prescribe therapy [15, 21]. Thus, the study may overestimate effectiveness or underestimate adverse effects.
Another potential methodological weakness is the small number of participants despite the four-year study. The fact that the study was conducted only in one country, thus limiting the scope of results, was on purpose and may reflect the reality of a specific geographic region. Additionally, the results of this real-world observational study may not have reflected all of the preferences of the panel of experts.
Altogether, this paper provides additional information on the effectiveness and feasibility of galcanezumab in CH; the findings emphasize the use of this mAb as an effective agent in managing CH, especially eCH. The development of galcanezumab as part of a multidimensional treatment plan endorsed by consensus-based guidelines is a major step forward in the care of this highly morbid disorder. However, the findings discussed also reveal the need to keep researching more about the possibilities of long-term therapy to clarify adherence issues and tolerability as well as the real need for combining treatments.


留言 (0)