
記住我
The Korean National Health Information Database is a public database provided by the Korean National Health Insurance Service (NHIS) and contains data on national health examination, medical treatment and insurance claims information, health care use, sociodemographic information, and mortality of the entire South Korean population since 2001 [15, 16]. The NHIS is a sole insurer and a mandatory universal public health insurance system that covers 97% of the Korean population. A medical aid is a public assistance that covers the remaining 3% of the population in the lowest income bracket; however, the NHIS also takes care of all the administrative processes for medical aid beneficiaries.
The NHIS has provided a national health examination program for the prevention and early detection of diseases since 1995 [17]. Until 2018, all adult employees or adults aged ≥ 40 years with national health insurance received a national health examination every other year (every year for manual workers), including simple chest radiographs, laboratory tests, and self-report questionnaires concerning lifestyle behaviors and medical history [16, 18].
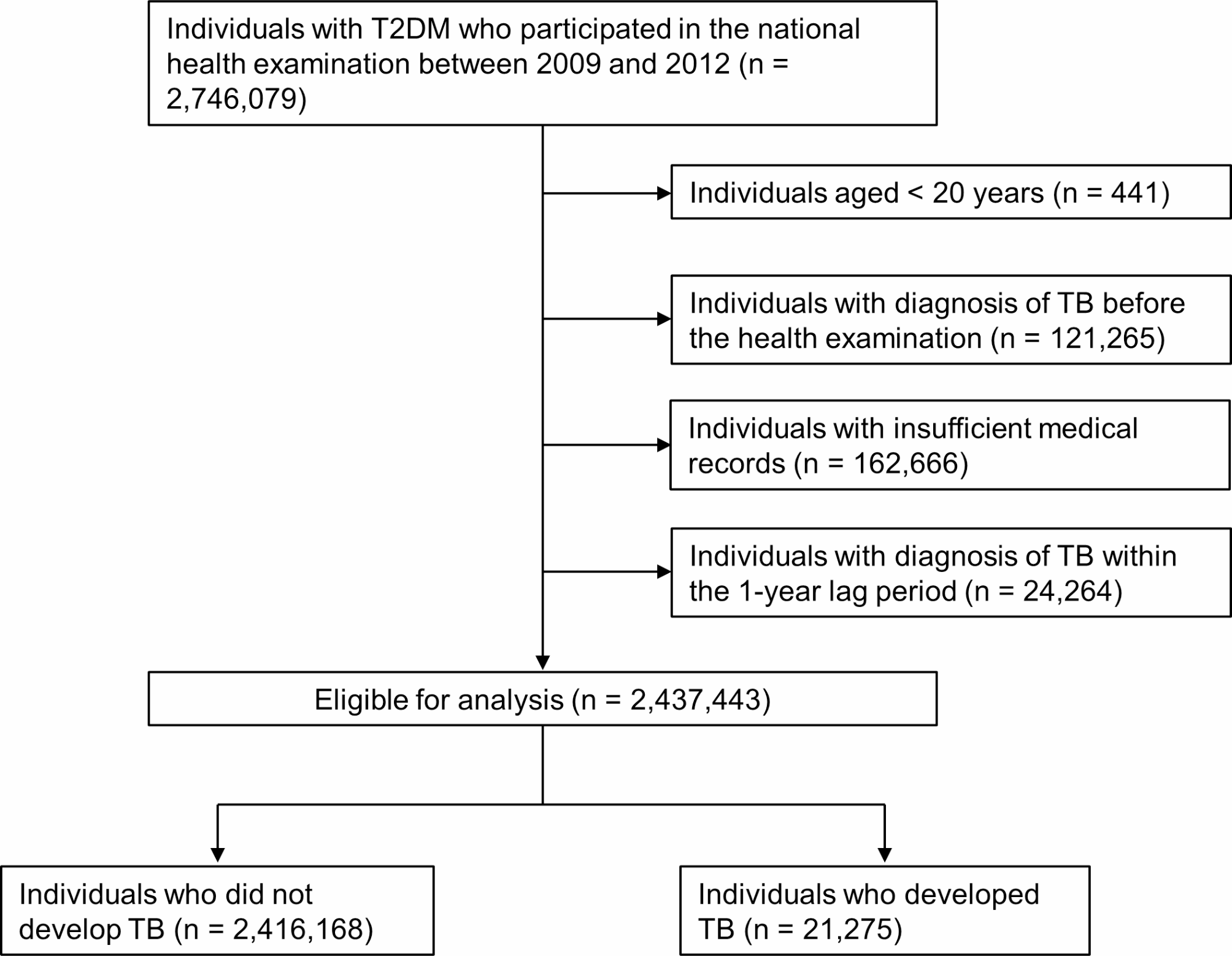
Study populationA total of 23,452,862 individuals who received a national health examination between 2009 and 2012 (the index year) were initially screened. Among them, we identified 2,746,079 individuals with T2DM according to the following operating definition: (1) insurance claim with International Classification of Diseases 10th Revision (ICD-10) codes for T2DM (E11–E14) with at least one prescription of oral hypoglycemic agents (OHAs) or insulin within a year before the health examination or (2) fasting blood glucose (FBG) concentration ≥ 126 mg/dL in the health examination data [14, 19, 20].
Thereafter, we excluded 441 individuals aged < 20 years, 121,265 individuals with any insurance claim with ICD-10 codes for TB (A15–19) before their health examination (TB wash-out), 162,666 individuals with insufficient medical records, and 24,264 individuals identified with TB according to the rare intractable disease (RID) registry (codes V206, V246, and V000) within 1 year after the index date (1-year lag period). The 1-year lag period was applied to exclude the overdetection of TB after the health examination. Finally, the remaining 2,437,443 eligible individuals with T2DM were included and started follow-up 1 year after the index date (time zero).
Study outcome: TB diagnosisThe outcome of this study was new TB development, which was identified using the RID registration codes for TB (V206, V246, and V000). Since 2005, the NHIS has provided a special copayment reduction (90–100%) for all patients with TB along with the national TB control policy. Attending physicians are obliged to report all newly diagnosed TB cases to nearby public health centers and register them in the RID program. Thereafter, TB cases are reviewed by the NHIS to provide copayment reduction. Under the current national TB reporting system, the RID registration codes for TB are valid measures to identify individuals with TB in the Korean population [14, 20, 21].
The study cohort were followed up until December 31, 2018, and the follow-up ended at TB development (outcome), death, or censor (e.g., out-migration). The mean follow-up duration was 6.87 ± 1.60 years, and 21,275 individuals were newly identified with TB according to the RID registry data (Fig. 1).
Fig. 1 Main exposure: alcohol consumption
Main exposure: alcohol consumptionAlcohol consumption information was collected from self-reported questionnaires during the national health examination within 2 years before the index date. The parameters obtained were the average frequency of alcohol beverage intake per week and the average number of drinks per occasion. A drink of beer, soju (Korean traditional alcohol beverage), wine, or whiskey corresponded to 8 g of pure alcohol [22]. The total alcohol amount consumed per week was calculated as 8 g of pure alcohol × number of drinks per occasion × frequency per week. By dividing 7 days, a daily alcohol intake was calculated. Based on this information, the participants were classified into three groups, viz., (1) nonalcohol drinkers: 0 g of alcohol per day; (2) mild-to-moderate alcohol drinkers: 1–29.9 g of alcohol per day; and (3) heavy alcohol drinkers: ≥30 g of alcohol per day.
CovariatesInformation on anthropometric measurements (body weight, height, and blood pressure) and lifestyle behaviors (cigarette smoking and physical activity) from self-reported questionnaires was collected during the national health examination within 2 years before the index date [23, 24]. Body mass index (BMI) was calculated by dividing body weight by height squared (kg/m2) [25]. Cigarette smoking was categorized into never, former, and current [14, 26]. Regular exercise was defined as > 30 min of moderate physical activity at least five times per week or > 20 min of vigorous physical activity at least three times per week [14, 21, 27]. The household income level was categorized into quartiles (Q1 = the lowest and Q4 = the highest) based on subscribers’ annual national health insurance premium. Medical aid beneficiaries were included into Q1 category [28].
Comorbidities were identified based on the NHIS and national health examination data within 1 year before the index date according to the following definitions: (1) hypertension, either an insurance claim for ICD-10 codes I10–13 and I15 with a prescription of antihypertensive medications or high blood pressure (systolic blood pressure ≥ 140 mmHg or diastolic blood pressure ≥ 90 mmHg) measured during a health examination; (2) dyslipidemia, either an insurance claim for ICD-10 code E78 with a prescription of lipid-lowering medications or serum total cholesterol ≥ 240 mg/dL measured during a health examination; and (3) chronic kidney disease (CKD), either an insurance claim for ICD-10 codes N18–19 or an estimated glomerular filtration rate < 60 mL/min/1.73 m2 calculated using the modification of diet in renal disease equation during a health examination [29].
Statistical analysisContinuous variables are expressed as mean ± standard deviation, and categorical variables are expressed as numbers (percentage). Student’s t-test and χ2 test were used to compare continuous and categorical variables, respectively. The TB incidence rate was calculated as the ratio between the number of patients with newly diagnosed TB and the number of person-years at risk of developing TB (per 1,000). The Kaplan–Meier analysis was used to calculate the cumulative TB incidence according to alcohol consumption categories. A multivariate Cox proportional hazards model was used to evaluate the effect of risk factors on the time-to-event of TB development. The proportional hazards assumption was checked using the Schoenfeld residuals test. Model 1 was nonadjusted. In Model 2, the covariates included age and sex. Model 3 included the covariates in Model 2 and BMI, income, cigarette smoking (non, former, current), regular exercise, hypertension, and dyslipidemia. Model 4 (the main analysis model) contained the covariates in Model 3 and FBG concentration, CKD (DM-related renal complication), T2DM duration (< 5 vs. ≥5 years), numbers of OHAs (< 3 vs. ≥3), and insulin. The last covariates were included as surrogate markers for DM severity, which was also associated with the risk of developing TB [20]. Subgroup analysis stratified by age and smoking status was performed for Model 4. In the multivariate analyses, age, BMI, and FBG concentration were included as continuous variables. All P values were two-tailed, and statistical significance was set at P < 0.05. All statistical analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC, United States), and the PHREG procedure was used for the Cox proportional hazards model.
留言 (0)