
記住我
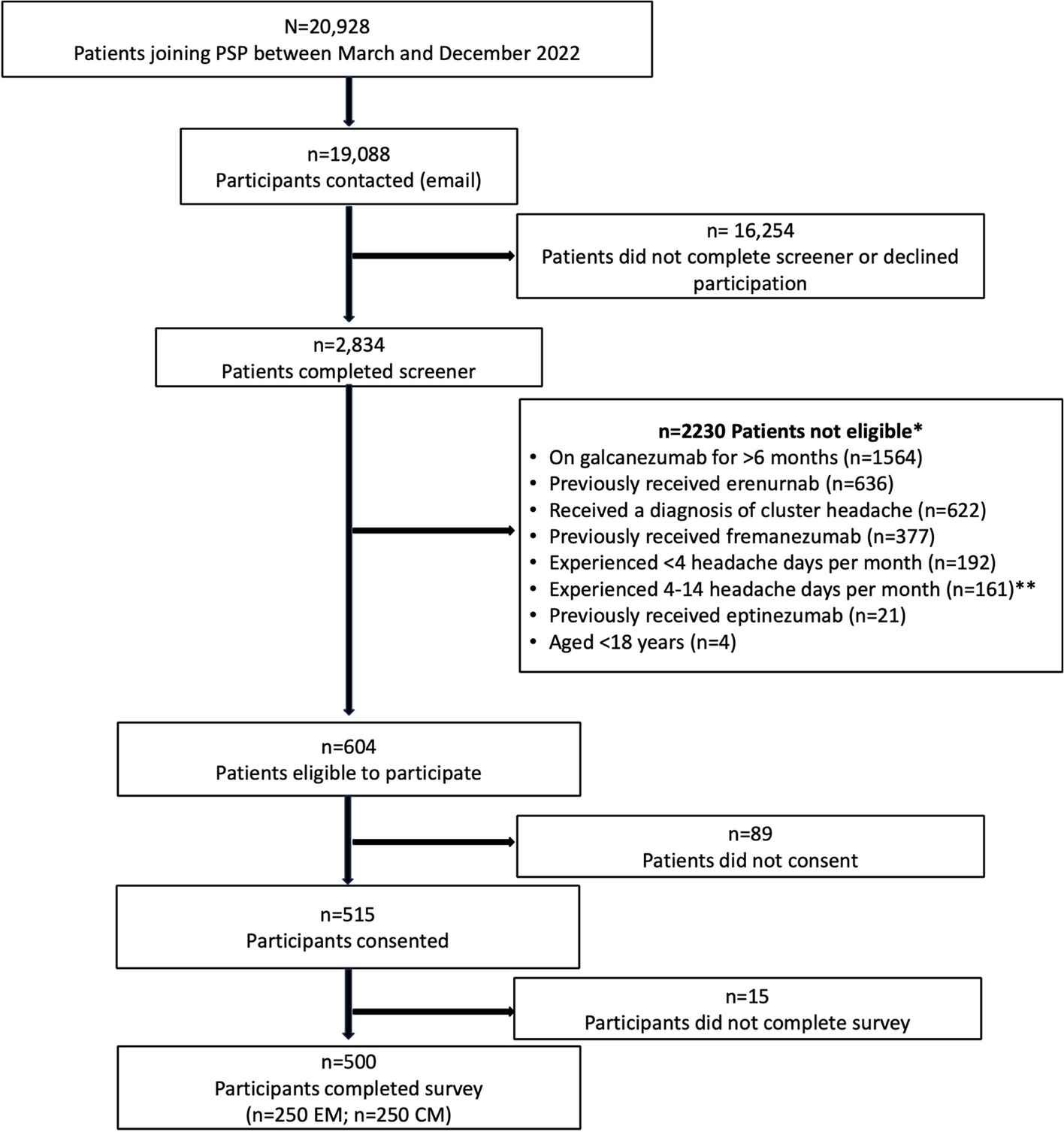
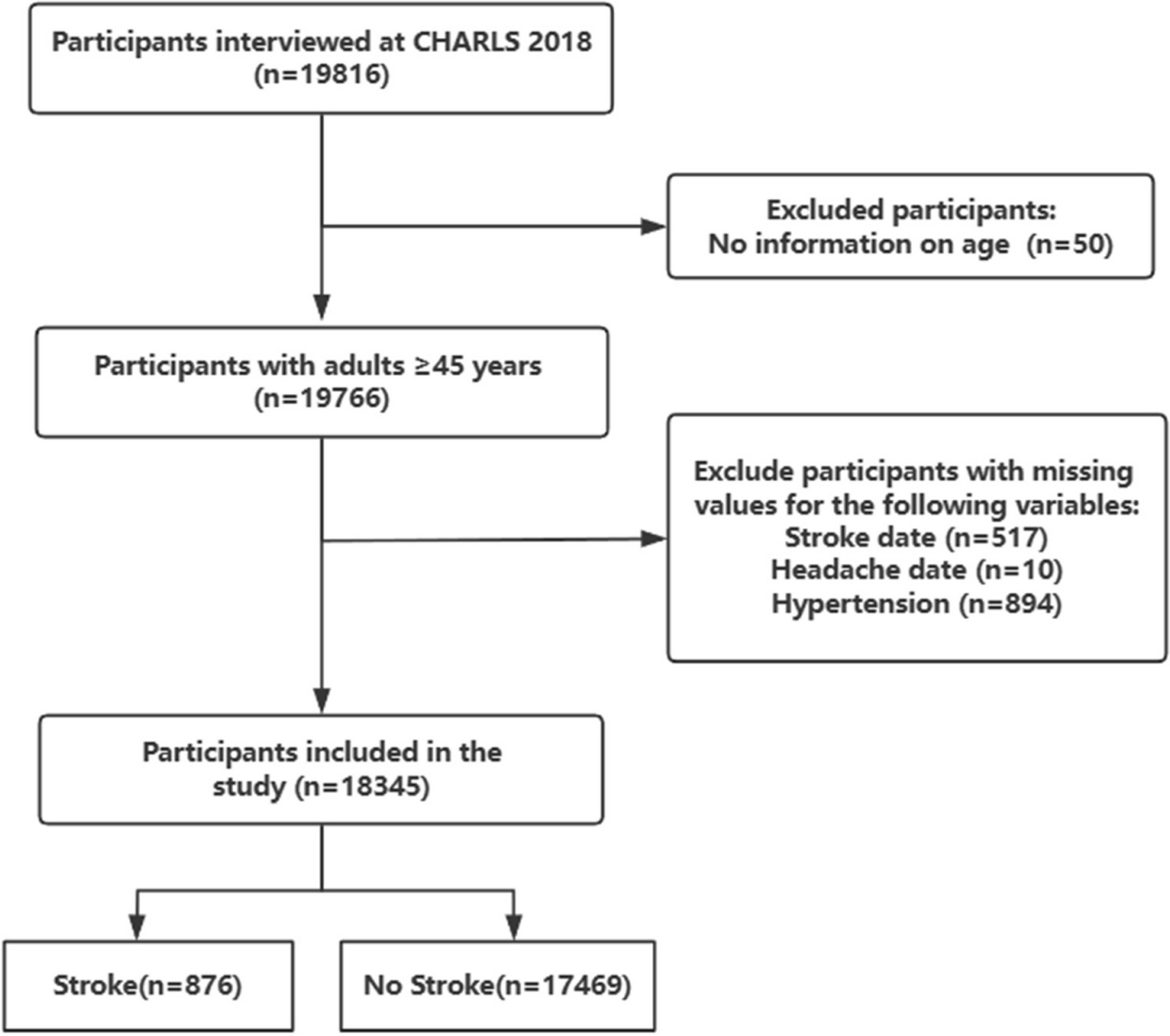

Data were derived from a prospective cohort study titled “Migraine Exposures and Cardiovascular Health in Hong Kong Chinese Women (MECH-HK)” [26, 27]. Initially, 4,221 women aged 30 years and older were enrolled between October 2019 and December 2020. Participants were eligible if they were free of cardiovascular disease at baseline. Between October 2021 and June 2023, approximately 1.27 years on average after initial enrolment, a follow-up assessment was completed by 3,451 participants. In this study, we included participants with complete CVH metrics and migraine status data at both baseline and follow-up. Participants were excluded if they ① had incomplete CVH metrics at either time point or ② had missing data on migraine status, sociodemographic information, or other relevant variables (Fig. 1).
Fig. 1
Data collection and screening flowchart for analysing the relationship between migraine and CVH profile changes in the MECH-HK cohort study (October 2019 - June 2023)
Sociodemographic, lifestyle, and health-related information were gathered via face-to-face questionnaires conducted through trained research assistants. Additionally, physical examinations and blood tests were performed to obtain biometric data. Informed consent was obtained from all participants, and ethical approval was granted by the Human Research Ethics Review Committee of the Hong Kong Polytechnic University (Reference: HSEARS20171229004) [26, 27].
Assessment of the cardiovascular health (CVH) profileThe CVH profile was assessed using a metric consisting of eight components adapted from the LE8 framework [9]. These components included dietary habits, physical activity (PA), nicotine exposure, sleep duration, BMI, lipid levels, blood pressure levels, and stress levels. Fasting blood glucose was excluded due to data unavailability. Stress was incorporated considering its growing acknowledgment as a key factor in CVD risk [13, 14].
Dietary habits were assessed through a questionnaire that assessed participants’ consumption frequency across eleven food groups in the previous month [27]. The food groups covered vegetables, fruits, dairy products (including cheese), soy products, eggs, meats, seafood, fish (excluding salted fish), cured meats, cakes, and preserved vegetables. The frequency of intake was classified as ‘never,’ ‘less than once a month,’ ‘1–3 days each month,’ ‘1–3 days each week,’ ‘4–6 days each week,’ and ‘daily.’ Foods such as fish, seafood, bean products, vegetables, and fruits were considered healthy for cardiovascular [28] and were scored from 0 to 5, with higher scores for more frequent intake. Conversely, preserved vegetables, cheese, cured meats, and cakes were considered unhealthy and were scored from 5 to 0 for more frequent consumption. Eggs and meats were excluded from the dietary metric due to the unresolved effect of eggs on cardiovascular risk [29] and the lack of distinction between red and non-red meats in our data, which have conflicting impacts. The total dietary score was derived by adding up all individual component scores, with higher values indicating more healthful dietary habits. These raw scores were then adjusted to a 100-point scale based on quantiles defined by the LE8 scoring criteria [9], with specific scoring details provided in Table 1.
Table 1 Distribution of CVH metric scores from baseline to follow-up in migraineurs and non-migraineursWe quantified PA via the International Physical Activity Questionnaire (IPAQ) [30]. To calculate a weekly total, moderate activity minutes were recorded as 1 unit, and vigorous activity minutes were weighted as 2 units. PA scores ranged from 0 to 100 points, with ≥ 150 min per week corresponding to 100 points, and 0 min corresponding to 0 points. Intermediate ranges aligned with the LE8 framework (Table 1).
Nicotine exposure was measured through self-reported cigarette use or second-hand exposure. Current smokers scored 0 points, non-smokers scored 100 points, and former smokers were assigned intermediate scores according to the LE8 criteria. Sleep health was measured via participants’ reported average sleep duration per night. As defined by the LE8 framework [9], a sleep duration of less than 4 h scored 0 points, while a duration of 7 to less than 9 h scored 100 points, with other durations assigned intermediate scores.
BMI was obtained as weight (kg)/height2 (m2). Individual’ height was assessed barefoot utilizing a stadiometer, whereas weight was assessed by the Inbody 270 body composition analyser, ensuring the removal of bulk clothing and accessories. The Chinese BMI scoring standards were applied, with a BMI of ≥ 35.0 scoring 0 points, a BMI of < 23 scoring 100 points, and other values receiving intermediate scores.
Blood lipid levels were evaluated using non-HDL cholesterol and scored based on the LE8 criteria. For individuals managing cholesterol levels with medication, an additional 20 points were deducted from their score. Blood pressure was assessed using both systolic and diastolic readings. Optimal levels (< 120/<80 mmHg) scored 100 points, while readings of ≥ 160 or ≥ 100 mmHg scored 0 points, with intermediate values assigned according to the LE8 framework. For participants with treated hypertension, an additional 20 points were deducted from their score.
Stress was assessed using the widely validated Perceived Stress Scale (PSS) [31], where participants rated 14 items on a scale from 0 (“not at all”) to 4 (“very frequently”). The overall PSS score was calculated by summing these item scores, resulting in a total score range of 0 to 56, with higher scores indicating greater perceived stress. For integration into the CVH metric and alignment with the LE8 framework, raw PSS scores were converted to a 0–100 scale: scores of 0–10 were allocated 100 points, 11–20 were allocated 75 points, 21–30 were allocated 50 points, 31–40 were allocated 25 points, and scores above 40 received 0 points, as detailed in Table 1.
In summary, each component was assigned a score on a 0-100 scale, and the overall CVH metric score was assessed by averaging the eight individual component scores. The overall CVH score, as well as the individual component scores, were classified into three levels: Low (0–49), Moderate (50–79), and High (80–100) [15]. Changes of the CVH profile were defined as shifts in these categories from baseline to the follow-up and were classified into three outcomes: “decrease”, “stable”, or “increase”. A decrease indicated that the CVH or individual component category at follow-up was lower than at baseline, while an increase represented an improvement. A stable outcome meant the category remained unchanged between baseline and follow-up.
Ascertainment of migraine and auraMigraine exposure was determined through a multi-step process, with detailed procedures provided in our previously published cohort profile [26]. Initially, participants were surveyed regarding their headache occurrences over the previous year via a structured questionnaire. Participants who responded with ‘Yes’ were then instructed to finish the ID Migraine™, a screening tool for migraine identification [32]. Participants who reported no headache occurrences were queried about any previous migraine diagnosis made by a physician. Individuals who either screened positive on the ID Migraine™ or reported a pre-existing diagnosis of migraine were classified as potential migraineurs. Participants who screened negative in the ID Migraine™ or lacked any prior diagnosis underwent additional evaluation to determine whether they had experienced migraine episodes at any point in their lifetime. This evaluation focused on identifying key symptoms, including phonophobia, photophobia, nausea, vomiting, or neurologic disturbances (e.g., visual flashes or tingling sensations) occurring within an hour before a headache. Participants who were confirmed to have experienced migraine attacks based on these criteria were also included as potential migraineurs [26]. A neurologist on our team carried out follow-up telephone interviews with these potential migraineurs to confirm the diagnosis. Based on the International Classification of Headache Disorders 3 (ICHD-3) [33], participants were classified into four categories: non-headache, non-migraine headache, probable migraine, and migraine. For the purpose of this study, individuals with either migraine or probable migraine were grouped as migraineurs, while those with non-migraine headaches or no headaches were assigned to the non-migraineur group. In the sensitivity analysis, participants who reported other types of headaches were excluded to assess the robustness of our results.
In accordance with the ICHD-3 criteria [33], migraine participants were categorized into those with aura and those without aura. Migraine with aura is defined by the presence of temporary neurological disturbances, including visual alterations, sensory disruptions, or language impairments, that precede the headache onset. Conversely, migraine without aura refers to migraine attacks that occur without these preceding neurological symptoms. In this study, individuals experiencing both types of episodes interchangeably were included in the “migraine with aura” group [26].
Ascertainment of other covariatesAll covariate data were collected through questionnaire assessment at baseline. Demographic and socioeconomic covariates included age, menopausal status, employment status, educational level, marital status, and household income. Age was treated as a continuous variable. Menopausal status was classified as “Yes” for post-menopausal participants and “No” for those who were pre-menopausal. Employment status was divided into two groups: participants employed full-time, part-time, or self-employed were categorized as “Yes,” while those unemployed for more than a year, recently unemployed (less than a year), retired, or unable to work were categorized as “No.” Education level was categorized into three subgroups: “Primary school or lower,” “Secondary school or pre-college,” and “College or higher.” Marital status was categorized as “Married or cohabiting” or “Never married, divorced, separated, or widowed.” Monthly household income was classified into three subgroups: “≤14,000 HKD/month,” “>14,000 and ≤ 35,000 HKD/month,” and “>35,000 HKD/month.”
In addition to the lifestyle factors analysed as part of the LE8 framework, we included two additional lifestyle factors as covariates: fatigue level and drinking status. Fatigue was measured using an 11-point self-perceived fatigue scale ranging from 0 (no fatigue) to 10 (most severe fatigue) [27]. Participants with scores at or above the median were categorized as having high fatigue [27], while those scoring below the median were considered to have no or low fatigue. Drinking status was divided into two categories: “Drinker” and “Never alcohol drinker.”
We included several disease-related covariates based on participants’ self-reported diagnoses and treatment status. These covariates covered cancer, hypertension, diabetes, and hyperlipidaemia. Hypertension status was categorized as “No hypertension,” “Hypertension treated,” and “Hypertension untreated.” Similarly, diabetes was classified as “No diabetes,” “Diabetes treated,” and “Diabetes untreated,” while hyperlipidaemia was grouped into “No hyperlipidaemia,” “Hyperlipidaemia treated,” and “Hyperlipidaemia untreated.” Cancer status was recorded as “Yes” for participants with a current or past diagnosis, and we assumed all participants with cancer would receive treatment. Those without any cancer diagnosis were recorded as “No.”
Statistical analysisBaseline characteristics were compared across subgroups based on migraine status (migraine versus non-migraine) and overall CVH categories (low, moderate, and high). Differences in continuous variables between migraine status groups were evaluated using two-sample t-tests, while differences across CVH categories were assessed using one-way ANOVA. Categorical variables were examined employing Chi-square tests or Fisher’s exact tests, selected based on appropriateness. For multiple comparisons across the three CVH subgroups (low, moderate, and high), Bonferroni correction was applied to control for Type I errors. This resulted in an adjusted significance threshold of p-value < 0.0167 (0.05 / 3), covering the three pairwise comparisons: low versus moderate, low versus high, and moderate versus high. To examine differences in the distribution of CVH metric scores from baseline to follow-up, we used Chi-square tests or Fisher’s exact tests, grouping the scores into four categories: <30, 30–50, 51–80, and > 80. Additionally, paired t-tests were utilized to evaluate changes in the continuous measurements of individual CVH components (e.g., blood pressure, cholesterol) between the two time points.
Multinomial logistic regression analyses were conducted to assess the impact of migraine on changes in CVH profiles from baseline to follow-up. Four models with progressive adjustments were used: ① Model 1 (unadjusted) evaluated the crude association between migraine and CVH changes without adjusting for any covariates; ② Model 2 adjusted for age only; ③ Model 3 further adjusted for multiple factors, including age, menopausal status, educational level, employment situation, marital status, household income, fatigue level, and drinking status; ④ Model 4 (fully adjusted) included all covariates from Model 2 and 3, along with additional disease-related variables, including cancer, hypertension, diabetes, and hyperlipidaemia. These analyses were conducted for both the overall CVH profile and each individual CVH component.
To further explore whether the impact of migraine on changes in overall CVH categories varied across subgroups, we conducted both subgroup and interaction term analyses, adjusting for relevant covariates. In the subgroup analysis, we stratified the dataset into groups based on various socioeconomic factors (including age, marital status, education level, employment status, and household income), women’s menopausal status, and disease-related factors (including cancer, hypertension, diabetes, hyperlipidaemia). Separate analyses were performed for each subgroup, and we calculated subgroup-specific odds ratios (ORs) to assess how migraine’s effect on CVH progression differed across these groups. We then used the entire dataset to build a full model with interaction terms to formally test the significance of interaction effects. Combining stratified analyses with interaction term modelling provided a better understanding of potential heterogeneity in the impact of migraine across different population subgroups.
Several sensitivity analyses were undertaken to confirm the results’ reliability. First, we adjusted the weights of the overall CVH score by grouping the eight components into two clusters: lifestyle components (dietary habits, PA, nicotine exposure, sleep duration, and stress) and clinical components (blood pressure, BMI, and lipid levels). In the main analysis, equal weights were assigned, with 50% allocated to lifestyle components and 50% to clinical components, and each of the eight individual components contributing equally to the final CVH score. For the sensitivity analysis, we explored several alternative weighting schemes, including 60% lifestyle and 40% clinical, 70% lifestyle and 30% clinical, 40% lifestyle and 60% clinical, and 30% lifestyle and 70% clinical. Second, participants who reported other types of headaches at baseline were excluded from the non-migraineur group. Third, changes in the CVH profile were evaluated using crude scores rather than categorical CVH classifications to define “increases” or “decreases.” Statistical significance was defined by a two-sided p-value < 0.05, and data were analysed utilizing R (version 4.1.2).
留言 (0)