
記住我
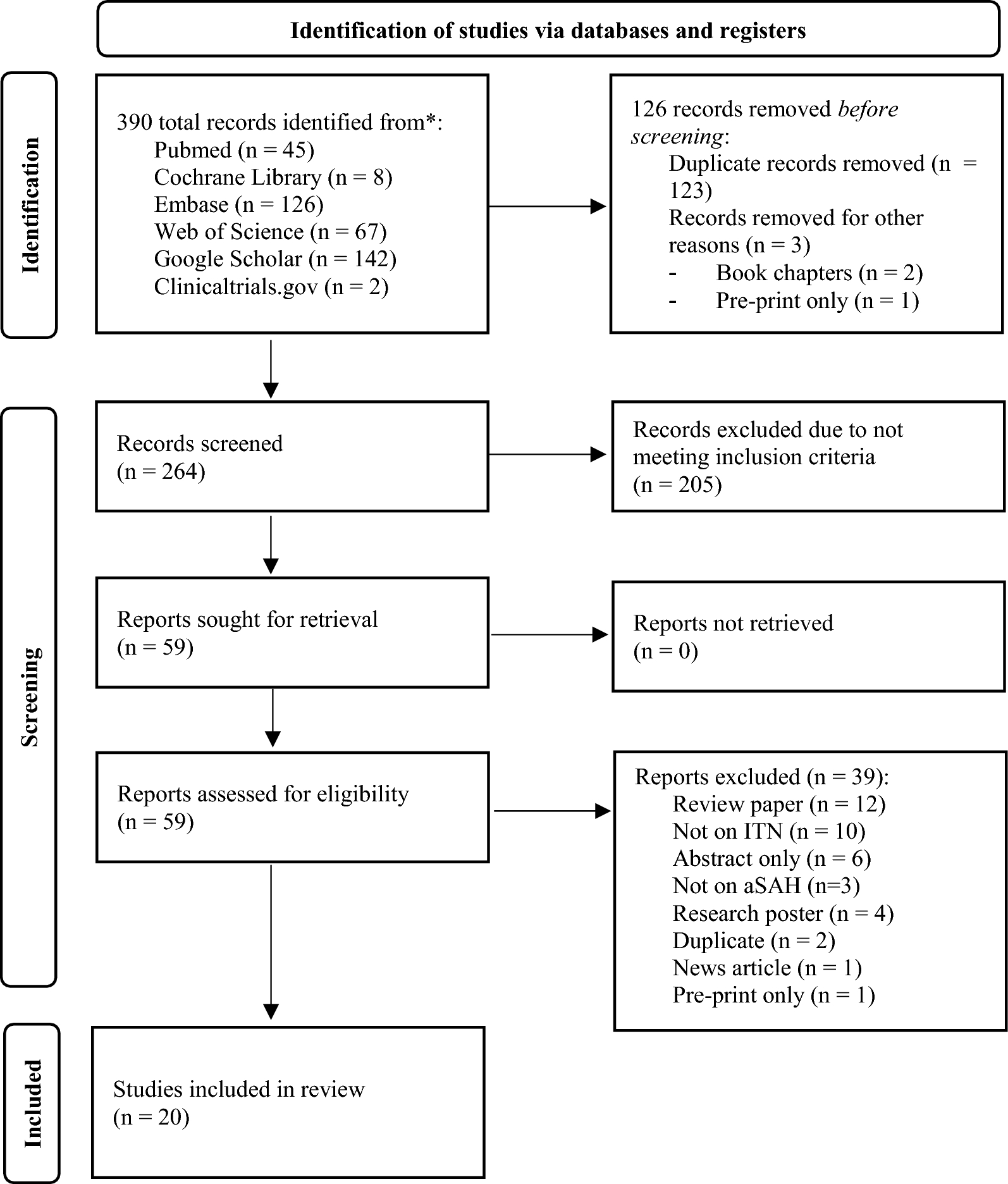

Following the search, 273 references were imported to Covidence for screening. After deduplication, the titles and abstracts of 156 articles were reviewed and 82 articles proceeded to full-text review. Sixty-two articles were ineligible and one article that met selection criteria was excluded [28], as this article described further analysis of previously reported data that were already included [30]. Full texts were unable to be sourced for two articles despite attempts to contact the authors directly. A total of 20 studies were included for review (Fig. 2) [7, 8, 30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47].
Fig. 2
PRISMA flow diagram. CINAHL – Cumulative Index to Nursing and Allied Health Literature; PRISMA—Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Study CharacteristicsThe 20 prospective observational studies were conducted in either general ICUs (n = 11; 55%) [8, 30, 32,33,34, 36, 37, 42,43,44,45] or neuroscience ICUs (n = 9; 45%) [7, 31, 35, 38,39,40,41, 46, 47] where patients were recruited consecutively on ICU admission. There were 3,965 participants across the 20 studies, and sample sizes were generally small, ranging from 55 [36] to 1,645 [45]. The study with the largest sample (N = 1,645) was the only study to conduct a priori power analysis [45]. The remaining studies had samples of 300 patients or less, seven of which reported samples with less than 100 patients [34, 36, 38, 39, 42, 44, 46]. Three studies only included patients with specific neurological illnesses: stroke of any etiology [35], ischemic stroke [37], and aneurysmal subarachnoid hemorrhage [38]. Another four studies included patients with any acute neurological condition [34, 39, 41, 47], and three studies only included patients with low GCS (≤ 9) [8, 31, 42]. Nine studies excluded patients who were sedated [7, 8, 33, 35, 40, 41, 43, 46, 47], and two studies only included patients after cardiac arrest [32, 44]. Most studies assessed GCS and FOUR score at least once within 24 h of admission [9, 27, 28, 30,31,32,33,34,35,36, 38,39,40,41,42,43,44], as shown in Table 1. Five studies assessed FOUR and GCS scores on multiple occasions at various time intervals [32, 35,36,37, 44].
Table 1 Study CharacteristicsQuality Assessment FindingsQuality assessment using the QUIPS tool [25] found 12 studies (60%) to have moderate overall RoB [7, 8, 31, 33, 37, 38, 41, 42, 44,45,46,47] and eight studies (40%) had high RoB [30, 32, 34,35,36, 39, 40, 43]. Risk of bias due to confounding (QUIPS Domain 5) was the most common reason for higher RoB scores, primarily due to a lack of adjustment for other prognostic factors. Methods for index and outcome measure assessment and data collection (QUIPS Domains 3 and 4) were often poorly described, therefore, it was difficult to ascertain how reliability was optimized. A traffic light plot and summary plot of RoB assessment findings are provided in Supplementary File 2.
Patient CharacteristicsMean age ranged from 40.1 [43] to 70.5 [
留言 (0)