
記住我

In 1856, Gubler called attention to the diagnostic importance of the so called alternate hemiplegia, which has been recognized as characteristic of any lesion of the pons [7]. The clinical picture of pontine hemorrhage matured and settled gradually although descriptors were already easily found in the early works [8, 9]. These were (1) sudden onset, (2) immediate respiratory compromise and apneic spells, (3) motor posturing, (4) hyperthermia in moribund states, and (5) poor outcomes. Mickle found vomiting, inability to swallow and “curious convulsive and twisting movements of the body.” He also emphasized sudden death, previously seen as not typical of any type of stroke [8, 9]. In 1877, Bode, in an inaugural thesis, published at Würzburg, collected the histories of 67 cases and contributed several of his own cases. This thesis became of much value to later clinicians [10]. He noted: “Der Anfall selbst geschieht fast immer plötzlich. (The attack itself happens almost always suddenly.) Wie vom Blitz getroffen. (As if hit by lightning) Das Bewusstsein ist verloren, die Glieder schlaff, die Respiration angestrengt, geräuschvoll, die Pupillen starr und verengt. (Consciousness is lost, the extremities are limp, breathing is strained and noisy, and pupils are fixed and constricted) Bisweilen beobachtet man auch während des Anfalls convulsivische Zuckungen von verschiedener Dauer und Intensität. (Sometimes you observe during the attack convulsive twitches of various duration and intensity),” and he emphasized that this may very much look like a seizure.
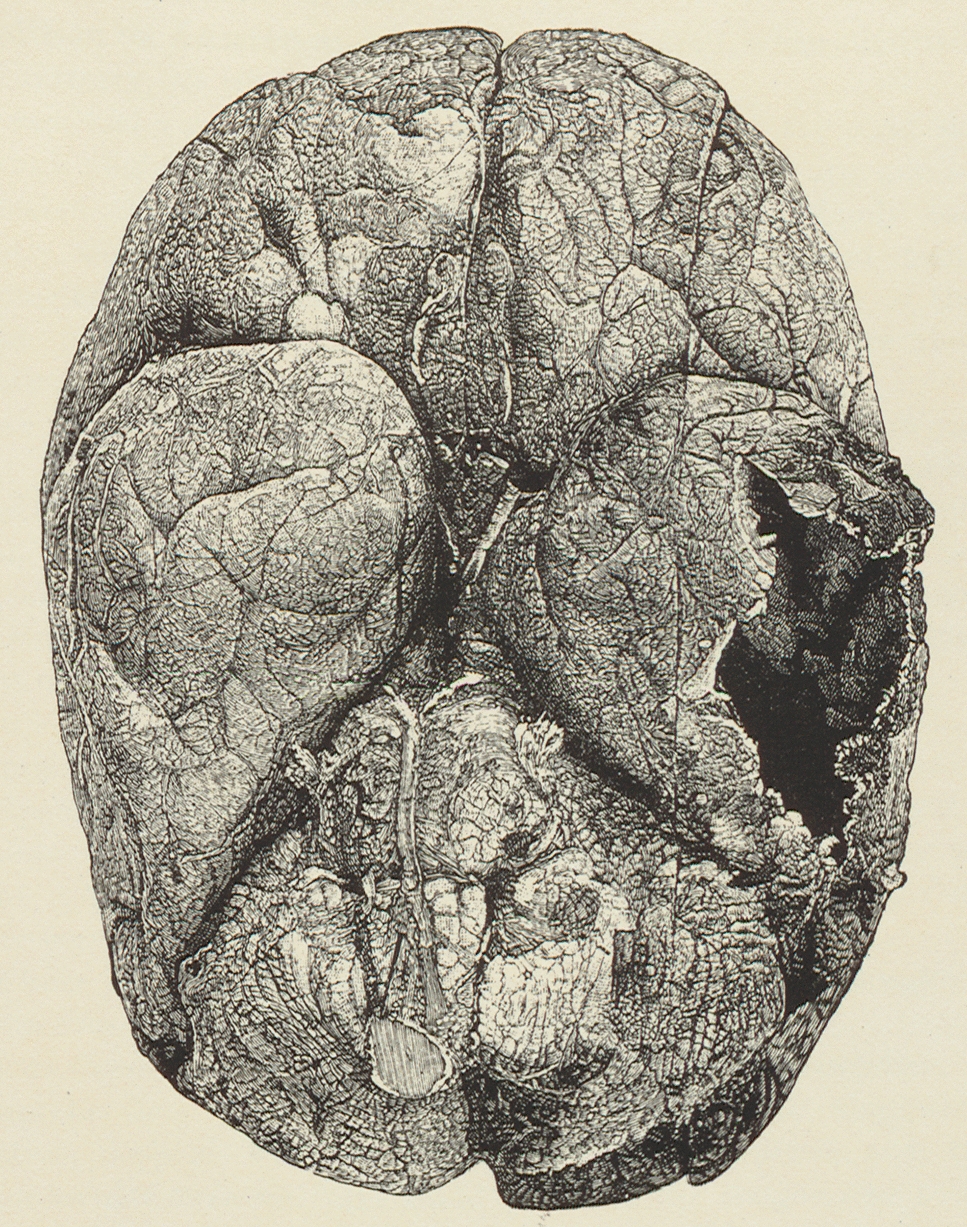
There was considerable interest in the convulsions associated with pontine hemorrhages and several authors attempted to explain it. In 1899, Dr. Hans Luce collected a series of 18 cases of pons hemorrhage and studied them to answer the question of convulsions produced by pons lesions [11]. These “epileptic attacks” were first noted by Ollivier d'Angers in his Traité de la moelle épinière published in 1827. However, it is Nothnagel who postulated a “cramp center” in the pons near the fourth ventricle; a circumscribed place, which would cause the tonic or clonic convulsions [12] (Fig. 2). None of them believed these were epileptic, although they very much looked like it. It remains unclear what these earlier clinicians meant, and it is possible all were looking at extensor posturing or some forme fruste mimicking seizures and confusing clinicians. Nothnagel was quite detailed in his description:
The patient lay on his back-all four limbs were absolutely flaccid and motionless; when held up they dropped back on the bed. Both eyes were directed downwards and a little to the right; the pupils were small, but not pin-point, and did not react to light. The left naso-labial furrow was a little deeper than the right; there was slight spasm of the muscles of the right side of the neck. The abdominal, cremasteric and plantar reflexes were absent. The knee-jerks were active, the right greater than the left; the elbow and ankle-jerks were present. The breathing became gradually slower and more labored, and the temperature steadily rose until it reached 110 degrees at his death at 7.30 p.m. on the same evening. There were no convulsions at any time [12].
Fig. 2
Nothnagel and his article
A series by Dinsdale summarized 20 cases of pontine hemorrhage and also emphasized elevated temperatures in comatose patients found with pinpoint pupils [13], a clinical sign that was corroborated by others later [14].
More details came from C. Miller Fisher, who added “ocular bobbing” (“the downward movement of the eyes is quicker than the upward, and between jerks the eyes are at rest”) and he also noted “It is released by extensive pontine lesions and does not occur in bilateral hemispheral disease or tentorial pressure coning” He did not see ocular bobbing with cerebellar hemorrhages, except in one case [15].
留言 (0)