Study design
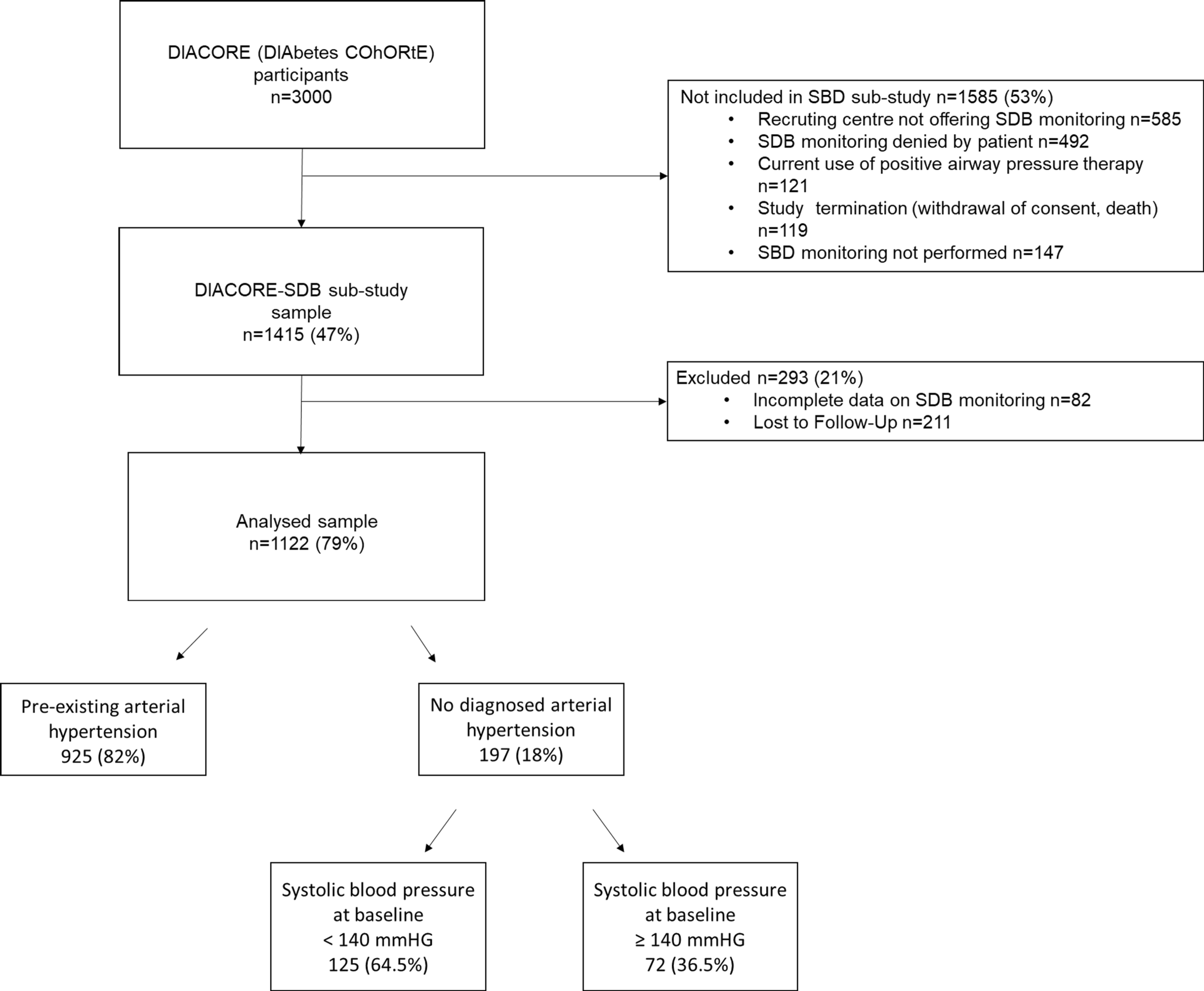
The DIACORE (DIAbetes COhoRtE) study is a prospective cohort study of 3000 participants with T2D conducted at two university hospital centers in Germany [17, 18]. Its design and protocol have been described in detail previously [17]. From 2010 to 2014, recruitment of participants took place through a variety of methods [17]. T2D was defined as a fasting plasma glucose level of ≥ 126 mg/dl in at least two measurements or a 2-hour glucose value in the oral glucose tolerance test of > 200 mg/dl and the need for blood-glucose-lowering medication [17, 19]. During the study, participants were interviewed using a standardized online questionnaire and underwent blood sampling and physical examination [17]. Anthropometric parameters (height, weight, waist-to-hip ratio) were measured in light clothing without shoes [17]. Obesity was defined as body mass index (BMI) ≥ 30 kg/m2 [20].
In 2011, the DIACORE sleep-disordered breathing (DIACORE-SDB) sub-study was initiated [18]. As part of this, participants underwent ambulatory polygraphy (Apnea-Link®; ResMed, Australia, Sydney) [17].
The protocol, data protection policy, and study procedures were approved by the ethics committees of the participating institutions and comply with the Declaration of Helsinki. Participation in the DIACORE study was confirmed by written informed consent of the participants [17]. The study is registered at the German Clinical Trials Register (DRKS00010498).
Study population
Inclusion and exclusion criteria of the DIACORE study have been described in detail previously [17]. For the DIACORE-SDB sub-study, participants had to consent for SDB monitoring and were not allowed to have existing treatment with nocturnal positive airway pressure (PAP) therapy [18].
High alcohol intake (≥ 3 drinks per week), smoking status, coronary heart disease (defined as coronary intervention, coronary bypass surgery, or myocardial infarction), physical activity (defined as light activity at least three times per week), and pre-existing aHT (defined as pre-diagnosed aHT or established antihypertensive medication) were evaluated by standardized questionnaires. Socioeconomic status was classified according to the German Robert Koch Institute [21] and subdivided into four groups ranging from 1 (lowest) to 4 (highest), taking into account educational level, professional qualification, and income.
Assessment of blood pressure and progression of arterial hypertension
Blood pressure was measured using a GE Dinamap Vital Signs Monitor, model V100 (Carescape, Germany) [17]. The cuff size was selected according to the participant’s upper arm circumference (either 23–33 cm or 31–40 cm) and placed at the heart level of the dominant arm [17]. After resting for at least 5 min in a sitting position, three blood pressure measurements were taken 2 min apart and the mean of the second and third values was used for the analysis [17].
Pathologic blood pressure values greater than 180/110 mm Hg or less than 90/50 mm Hg were reported to participants at the study visit [17]. Progression of aHT was defined as a systolic blood pressure of 140 mm Hg or higher at follow-up, accompanied by an increase of at least 10 mm Hg in comparison to the baseline visit.
Assessment of antihypertensive treatment and coronary artery disease
The participants’ medication intake was assessed through medical records and questionnaires. Antihypertensive therapy was determined according to whether the participant was taking any medication belonging to the following groups: diuretics, beta blockers, calcium antagonists, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, or renin antagonists. Coronary heart disease was assessed based on participants’ reports and validated by medical records.
Assessment of sleep-disordered breathing
Ambulatory polygraphy with a validated monitoring device (ApneaLink®; ResMed, Sydney, Australia) was performed to record airflow via nasal cannulae and pulse oximetry using a finger clip. This method has undergone validation in numerous studies concerning monitoring of SDB, as detailed previously [22,23,24].
The ApneaLink® device settings were used to define apnea, hypopnea, and desaturation [25]. Apnea was defined as a drop in nasal airflow of at least 80% for ≥10 s, hypopnea as a drop in airflow of 50–80% compared with baseline for ≥10 s followed by a drop in oxygen saturation of ≥ 4%, and desaturation as a drop in oxygen saturation of at least 4%. The results included the apnea–hypopnea index (AHI), the oxygen desaturation index (ODI), and the TSat90% (percentage of peripheral oxygen saturation below 90% during the entire recording period). Since chest straps were not used, it was not possible to distinguish between obstructive and central apneas. All participants were informed about the monitoring results, though no further diagnostics or treatment were part of the DIACORE study protocol [17]. Newly initiated continuous positive airway pressure (CPAP) therapy during the course of the study was documented in standardized questionnaires during follow-up examinations [17].
The validated Epworth Sleepiness Scale (ESS) was used to measure subjective daytime sleepiness. Participants were asked to rate the likelihood of falling asleep in various common situations (scores range from 0 as least sleepy to 24 as sleepiest) [18].
Statistical analysis
Statistical analysis of data was conducted with SPSS software (version 28.0.1.1; IBM SPSS Statistics, Armonk, New York, USA). Mean ± standard deviation (SD) was used to calculate descriptive data for normally distributed variables, while median and interquartile ranges were used for non-normally distributed variables. Categorical data were expressed in absolute numbers and percentages (%). The t‑test was used for normally distributed continuous variables, Mann–Whitney U test for non-normally distributed continuous variables, and chi-squared test for categorical variables. Univariate and multivariate binary logistic regressions were conducted to identify predictors of the progression of aHT. Risk factors for incident or progressive aHT, such as age, sex, BMI, T2D duration, systolic blood pressure, estimated glomerular filtration rate (eGFR), alcohol consumption, coronary heart disease, smoking status, physical activity, pre-existing aHT, and number of different antihypertensive agents were used as covariates. A p-value <0.05 was defined as statistically significant.





留言 (0)