This study conducted a survey targeting surgeons and anesthesiologists across multiple institutions to assess the awareness and challenges in prehabilitation. The results indicated that although awareness of prehabilitation is low, most surgeons and anesthesiologists recognize its necessity and widely support its importance. Several factors might have contributed to the low level of awareness in this field, including a lack of education, insufficient guidelines, and inadequate organizational support. These may significantly impact preoperative patient care and outcomes. The preoperative period is utilized to modify risk factors associated with physical status to increase physiologic reserve in an appropriate time window between diagnosis and surgery [9]. To optimize patients’ conditions before surgery, it is essential to raise awareness and understanding while also implementing organized efforts. Potential solutions include the development of educational programs, training sessions, and advocacy within healthcare organizations. However, despite the recognition of the need for these measures, various barriers to implementation remain. The most common reason was “the busy outpatient schedule makes it difficult to secure time to explain prehabilitation.” Given the challenges, it is difficult to request detailed explanations of prehabilitation from surgeons and anesthesiologists. In response to this, it is desirable to distribute explanations to patients via videos or pamphlets, promote multidisciplinary collaboration, and establish a contact point managed by co-medical staff. Creating an algorithm for patients who need prehabilitation, including order systems for referrals to nutrition departments and evaluations by physical therapists, is essential, necessitating multidisciplinary collaboration [10]. Prehabilitation enhances functional capacity before and after surgery, does not harm, and can be implemented for some types of cancer surgery with no age limit [11,12,13,14,15]. The specific components of the prehabilitation program are as follows: once surgery is scheduled, patients receive nutritional therapy, including guidance from a dietitian to correct nutritional deficiencies and ensure adequate protein intake. Exercise therapy focuses on increasing daily step count through aerobic exercise, such as walking. Psychological therapy involves the patient independently practicing relaxation techniques. Additionally, patients are advised to abstain from smoking and alcohol. Implementing prehabilitation to optimize preoperative conditions is highly beneficial for patients. Nutritional and exercise therapies are recommended, yet the implementation rate remains low worldwide [4,5,6]. Although prehabilitation has been shown to contribute to postoperative recovery and the reduction of complications, its implementation rate remains low. To address this issue, the introduction of simple explanatory tools and remote care options could be effective [16,17,18].
While patients were unaware that prehabilitation reduces postoperative complications, they believed that it promotes postoperative recovery [8]. Further, patients were more inclined to participate in prehabilitation programs if recommended by their physicians [8]. Surgeons and anesthesiologists who explain surgery and anesthesia to patients should also briefly recommend prehabilitation, as this can lead to increased implementation rates.
In our study, approximately 40% of surgeons indicated that it is possible to delay non-emergency surgeries to implement prehabilitation with the most commonly cited extension periods ranging 14–30 days. Previous studies have shown that many surgeons are willing to delay surgeries by 2–4 weeks for prehabilitation [6, 19]. These findings suggest that there is flexibility in surgical scheduling, and if surgeons recognize the effectiveness of prehabilitation in optimizing patient conditions, the preoperative period can be secured. ESPEN guidelines strongly recommend preoperative nutritional therapy for patients at high nutritional risk, even if it means delaying surgery [20]. Only 7% responded that it was impossible to coordinate with relevant departments after the surgery was decided. This result indicates that if a simple order system can be established, prehabilitation intervention can be initiated once the surgery is scheduled.
Recently, prehabilitation guidelines have been developed for patients with cancer, supporting not only the promotion of recovery but also long-term health behaviors that improve the quality of life and empower the patients [3]. This approach may also contribute to preventive medicine and can be regarded as a health-promoting behavior that should be incorporated into daily life. Prehabilitation programs indeed represent a teachable moment for lifestyle changes and provide a platform for shared decision-making based on a collaborative and holistic clinician-patient relationship [21]. Compared with the postoperative period, the preoperative period presents fewer restrictions on physical activity due to the absence of intravenous lines, pain, or environmental changes, providing an excellent opportunity for patients to gain self-efficacy in preparation for surgery. Nutritional and exercise therapies do not involve particularly difficult actions but promote healthy behaviors. It is important to support patients in enhancing their physical and mental health independently.
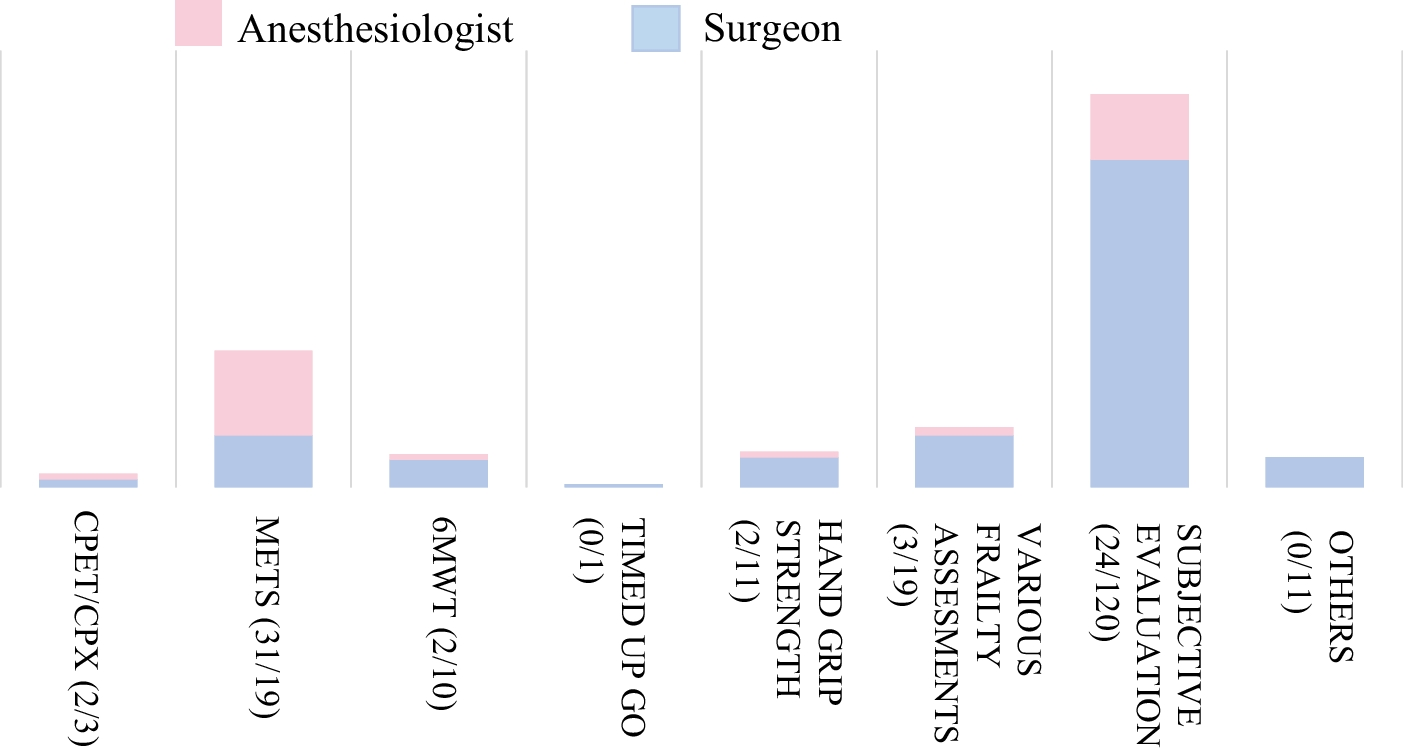
Regarding preoperative patient evaluation, anesthesiologists use the American Society of Anesthesiologists physical status classification to assess the severity of surgical patients [22]; similarly, the anesthesiologists in this multicenter study used this assessment preoperatively. However, 60.3% of surgeons did not use any assessment tools. The most common indicator for preoperative exercise tolerance was subjective assessment, used by 77% of respondents, showing a predominant reliance on non-objective measures. However, given the uncertain accuracy of subjective assessments of patient functional capacity, it is recommended to use screening tools rather than subjective evaluations for preoperative assessment [23, 24].
Although both exercise and nutritional therapy were primarily assessed subjectively in this study, combining useful assessment tools with subjective evaluations might better prepare the patients for surgery.
Limitations
This study has few limitations. First, the response rate of 61.7% indicates that the understanding and perceptions of 38.3% of non-respondents remain unknown, potentially reflecting a lack of acceptance of prehabilitation among non-respondents. However, previous surveys of surgeons reported response rates of 18.7% [6] and 14% [19], suggesting the present study’s results are relatively reliable. Second, there is a bias in the distribution of medical specialties, making it difficult to detect differences between subspecialties. Addressing this will require further large-scale, multi-institutional research. Third, this report shows the current situation in a limited number of areas and facilities in Japan rather than that in Japan as a whole. Finally, since the survey targeted only surgeons and anesthetists, future investigations should include related professionals such as nutritionists, physical therapists, and nurses, considering the multidisciplinary nature of prehabilitation.



留言 (0)