Severe PH complicates anesthetic management by potentially triggering a vicious cycle as follows: (1) worsening of right heart failure, (2) reduced forward flow to the left heart, and (3) decreased cardiac output and reduced coronary perfusion, further deteriorating right heart failure [4]. Therefore, the major goals of perioperative hemodynamic management for patients with severe PH include avoiding further elevation of PVR and maintaining cardiac contractility and systemic perfusion pressure.
Concerning abdominal surgeries, the choice of surgical approach may have a great impact on hemodynamics in patients with severe PH. In both of our cases, multidisciplinary discussions eventually led to the selection of the open approach over the laparoscopic approach. Despite previous reports demonstrating successful laparoscopic surgeries for patients with severe PH [5,6,7], the implementation of pneumoperitoneum in the laparoscopic approach potentially worsens PH through several mechanisms, such as abdominal distention, hypercapnia, acidemia, and reduced lung compliance [8, 9]. Although the invasiveness and postoperative pain associated with the open approach can be deleterious, these disadvantages were successfully overcome by postoperative epidural analgesia in both of our cases. Thus, an open approach can be an option for patients with severe PH provided that excellent postoperative pain control can be achieved with epidural analgesia.
Several predisposing factors have been proposed for predicting poor postoperative outcomes after noncardiac surgeries in patients with severe PH. These include age \(\ge\) 75 years, New York Heart Association functional classification \(\ge\) II, systolic PAP \(\ge\) 70 mmHg, CVP > 7 mmHg, emergency cases, and moderate-to-high-risk surgical procedures [10,11,12,13]. In the case of adult congenital heart disease with PH, various postoperative risk stratification models for noncardiac surgeries based on multiple factors, such as physical status, complexity of the cardiac lesion, age, other comorbidities, and risk of the surgical procedure, have also been validated [14]. Recently, Hassan et al. proposed a simple composite risk assessment tool for patients with PH undergoing noncardiac surgery that combines patient-level and procedural variables (Table 1) [15]. Based on these risk stratifications, our cases were both classified into the high-risk group.
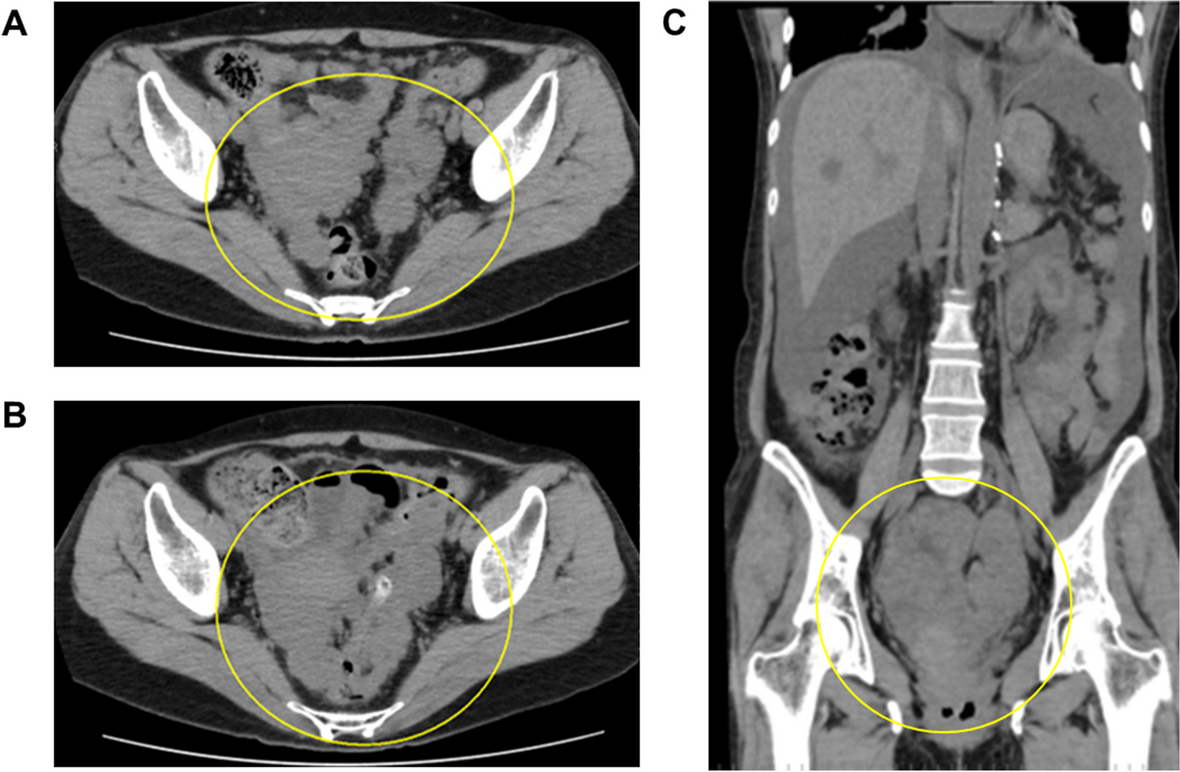
Table 1 A simple perioperative risk assessment tool for patients with pulmonary hypertension [15]Nevertheless, the pathology of PH can change dynamically in response to anesthetic and surgical interventions. As for adult congenital heart diseases with intracardiac shunts, such as in Case 1, a worsening of PH may increase the right-to-left shunt, immediately leading to systemic deoxygenation. Therefore, regardless of the preoperative risk estimation, close perioperative monitoring, including ABP, CVP, pulse oximetry (SpO2), PAP, and echocardiography, should always be considered in patients with severe PH. Although the aspiration of 15 L of intra-tumor fluid over 30 min did not result in major hemodynamic changes in Case 1, such a radical surgical maneuver should have been carefully performed with meticulous monitoring of the aforementioned hemodynamic parameters.
The choice of anesthetic method remains a topic of discussion for patients with severe PH. Although general anesthesia can provide excellent depth of sedation, muscle relaxation, and analgesia, the most commonly used general anesthetics have hemodynamically unfavorable effects on PH circulation, such as reductions in cardiac contractility, systemic vascular resistance (SVR), and preload [6, 16]. In addition, an increase in airway pressure caused by mechanical ventilation potentially aggravates PH by elevating the PVR [17]. Moreover, sympathetic responses associated with intubation and extubation may have detrimental effects on the PH circulation. However, some guidelines recommend not using spinal anesthesia in patients with severe PH because of concerns regarding rapid hemodynamic derangements, including the rapid reduction of SVR and preload [13, 18]. Despite these recommendations, the prophylactic use of phenylephrine infusion successfully counteracted spinal anesthesia-induced hypotension in Case 1. Hemodynamically, epidural anesthesia shares similar disadvantages with spinal anesthesia but generally has a milder and slower onset of sympathetic inactivation. However, in Case 2, a higher dose of phenylephrine and noradrenaline infusion were required to maintain the ABP. The severer PH in Case 2 (mPAP, 39 mmHg, PVR 3.5 Wood units in Case 1; mPAP, 65 mmHg, PVR 16.5 Wood units in Case 2) may have contributed to the more pronounced hemodynamic effects of neuraxial anesthesia.
Vasoactive drugs are often necessary to counter the hypotension associated with anesthesia in patients with severe PH. However, the selection of vasoactive drugs should be determined with special caution. In our case, maintenance of ABP was achieved with vasopressors, including phenylephrine and noradrenaline, without any signs of hemodynamic derangement. However, these vasopressors potentially disrupt circulation in PH by increasing PVR via the action of alpha-adrenergic receptors in the pulmonary vasculature [13]. Although there are few data, vasopressin can be an option in some cases of severe PH because of its systemic vasopressive effect without increasing PVR [3, 11]. The use of inotropes, including dobutamine, PDE-III inhibitors, adrenaline, and/or inhaled nitric oxide, should be considered in patients with progressive right ventricle dysfunction.
Collectively, although the use of vasopressors should be optimized depending on the severity, pathophysiology, and responsiveness to PH, neuraxial anesthesia may be an option for patients with severe PH undergoing abdominal surgery. Nevertheless, rigorous hemodynamic monitoring and multidisciplinary collaboration are mandatory for the safe perioperative management of patients with severe PH.









留言 (0)