We experienced a successful CSEA for a C-section of a patient with NF-1-associated dual ectasis. When performing neuraxial anesthesia in patients with NF-1, dural ectasia should be considered as a potential complication. CSEA can be a useful anesthetic option.
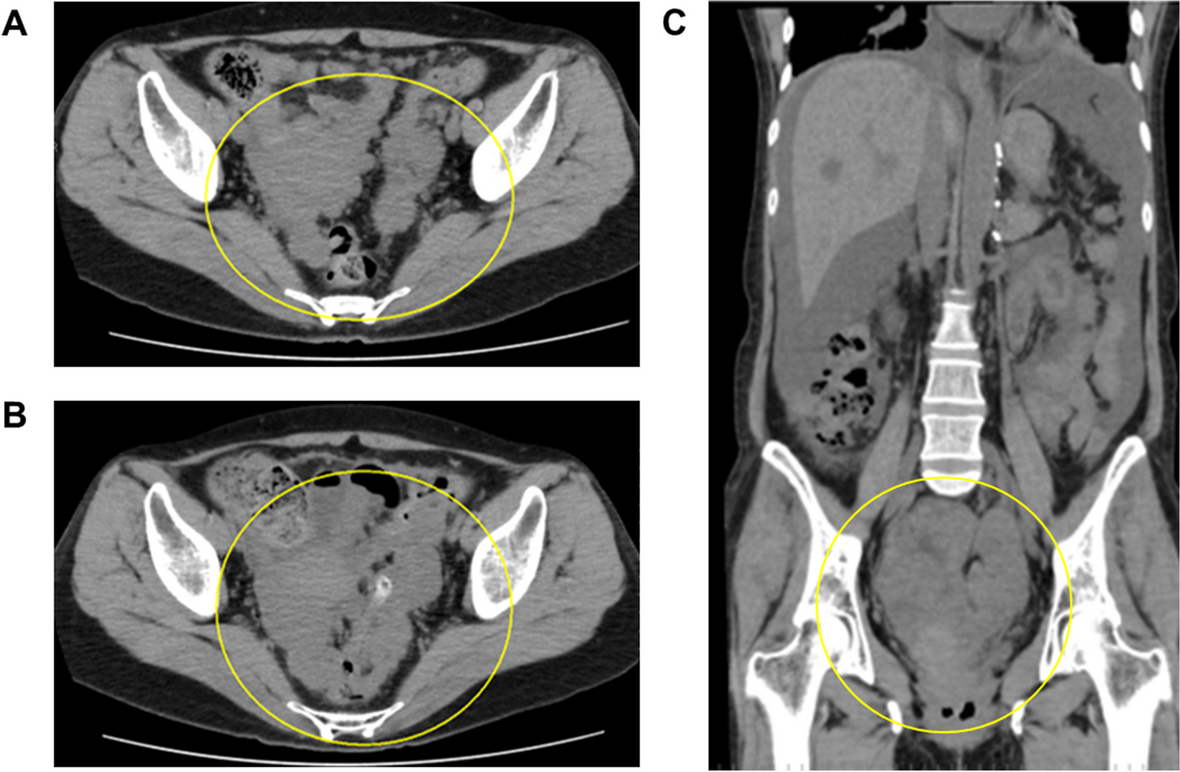
To the best of our knowledge, this is the first case report of spinal anesthesia failure in an NF-1 patient due to dural ectasia. Dural ectasia has been extensively described in Marfan syndrome, with its prevalence ranging from 63 to 92% [6, 7]. A previous review of NF-1 found a 25.7% incidence of dural ectasia [2], suggesting that it is not a rare manifestation of NF-1. In cases of dural ectasia, spinal anesthesia failure is considered to be caused by increased cerebrospinal fluid volume in the distended dural sac, which restricts the spread of intrathecally injected local anesthetic [4, 5]. The success of spinal anesthesia differs based on the extent of dural ectasia [8]. Based on the grading system developed by Fattori et al. [7], our patient, the MRI of whom revealed expanded dural sac and small radicular cyst, was classified as having mild dural ectasia. The present case showed that even the presence of mild dural ectasia does not guarantee the success of spinal anesthesia.
Case reports describing CSEA in patients with Marfan syndrome having dural ectasia are scarce [5, 8, 9]. These reports indicated that while spinal anesthesia failed to provide adequate block levels for elective C-sections, epidural anesthesia was successfully employed without complications. Epidural anesthesia is not an absolute contraindication in patients with dural ectasia; however, it requires careful consideration and skillful technique due to the increased risk of dural puncture in moderate-to-severe cases [8]. In our case, the MRI images facilitated the selection of CSEA.
In an NF-1 parturient, the necessity of neuraxial imaging before neuraxial anesthesia is controversial. During pregnancy, neurofibromas can increase in size [10], and the possibility of spinal tumor growth is a potential risk of neuraxial anesthesia. Older publications recommended avoiding neuraxial anesthesia in the absence of neuraxial imaging [11, 12]. Meanwhile, the practice guideline from the American College of Medical Genetics and Genomics states that preanesthetic neuraxial imaging is probably not required [13]. However, these recommendations do not mention dural ectasia. Patients with dural ectasia may present with low back pain, radicular pain in the buttocks or legs, or headache, but most, like our case, are asymptomatic [14]. The lack of neuraxial imaging may lead to oversight of asymptomatic dural ectasia. Therefore, we consider that neuraxial imaging is beneficial to enhancing patient safety when performing neuraxial anesthesia in NF-1 patients. In a patient with increased intracranial pressure caused by an enlarged intracranial tumor, neuraxial anesthesia can result in brain herniation [11]. In the present case, we did not perform brain MRI due to the absence of symptoms, such as headache, nausea, vomiting, and visual disturbances. If there are concerns, a brain MRI may be advisable for safety assurance.









留言 (0)