
記住我








This randomized, single-blind, cross-over study was performed at the intensive care unit of Gunma University Hospital from December 15, 2021, to July 26, 2022. This study conformed to the standards of the Declaration of Helsinki and was approved by the ethics committee of Gunma University Hospital (Trial No. IRB2021-042) on November 25, 2021. The study was registered with the University Hospital Medical Information Network Clinical Trials Registry (UMIN000046280) on December 6, 2021. Study participation was voluntary, and each patient gave their written informed consent for participation.
SubjectsInclusion criteria for study participation were (1) post-urologic surgery patients over 20 years of age scheduled for elective admission to the ICU after surgery, (2) legally competent to consent, and (3) scheduled for intraoperative and postoperative management with direct measurement of arterial pressure via an arterial cannula. Exclusion criteria were (1) history of respiratory illness, (2) American Society of Anesthesiologists physical status three or higher, and (3) determined by the physician as being ineligible for participation.
The criteria for discontinuation of the research were: (1) need for discontinuation, as judged by the physician in charge, due to the development of undesirable symptoms, (2) withdrawal of consent by the research subject, (3) decrease in the patient’s percutaneous oxygen saturation (SpO2) to below 91%, (4) decrease in PaO2 to below 60 mmHg, (5) increase of partial pressure of arterial carbon dioxide (PaCO2) to 55 mmHg or higher, (6) patient remaining intubated at the time of admission to the ICU, (7) cancellation of ICU admission, and (8) if the patient met any of the exclusion criteria.
Based on our pilot study, the required sample size was 32 subjects with power analysis using α = 0.05 and β = 0.8. Assuming a 25% dropout rate, 42 participants were enrolled in the present study.
EndpointsThe primary endpoint was PaO2 level five minutes after the change in oxygen delivery method, and the secondary endpoints were PaCO2 levels at the same time points.
Oxygen administration methodThe intervention was initiated when more than one hour had elapsed since the patient’s admission to the ICU and when the administration of 4 L.min−1 of oxygen was considered sufficient. Oxygen was administered at a flow rate of 4 L.min−1 with an oxygen mask (Japan Medicalnext Co. Ltd., Osaka, Japan, catalog No. 1135015) or oxygen cannula (Japan Medicalnext Co. Ltd., Osaka, Japan, catalog No. 001597). COMFORT + ® Level-1 (Medicom Japan Inc. Ltd., Kobe, Japan), which is the surgical mask we use in our daily practice and meets level 1 of the American Society for Testing and Materials (ASTM), was used as the surgical mask. This mask has a particle filtration efficacy (PFE), which is an indicator of the ability to collect particles 0.1 μm in diameter, of higher than 98%, indicating that it has sufficient performance to collect small particles.
Using the cross-over method, oxygen was sequentially administered by each of the following three methods (Fig. 1): via nasal cannula under the surgical mask, with an oxygen mask under the surgical mask, and via an oxygen mask over the surgical mask. All participants received oxygen once by each method. The order of administration was randomly selected from among six different ways using the envelope method (Fig. 2). In the envelope method, a piece of paper with the order of oxygen administration was placed inside the envelope, and oxygen was administered in the order indicated on the paper. This randomization allowed us to eliminate the potential risk of systematic error that might arise from fixing the order of oxygen administration methods. Randomization and patient assignment were performed by a single investigator (A.K.).
Fig. 1
The three different oxygen administration methods tested. The images show wearing a nasal cannula under the surgical mask (A), and wearing an oxygen mask under (B) and over (C) the surgical mask
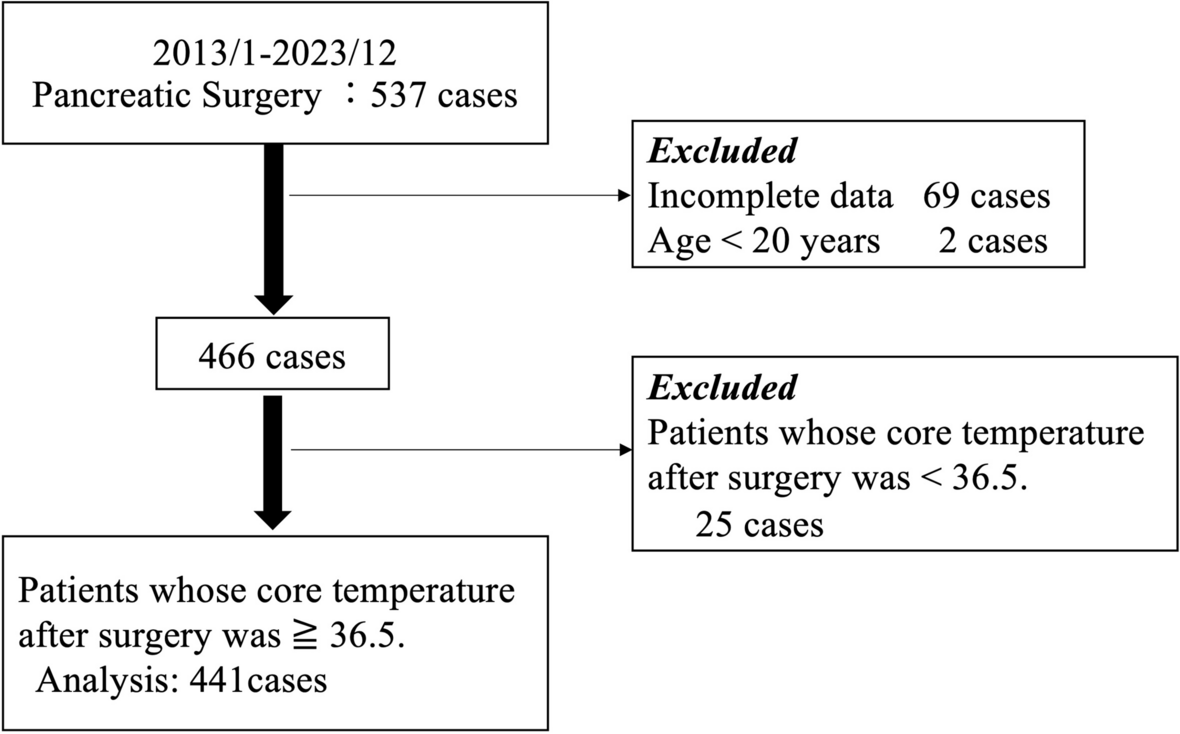
Fig. 2
Subject recruitment, randomization, and analysis
Measurement methodFive minutes after changing the oxygen administration method, arterial blood was collected via the arterial catheter, and PaO2 and PaCO2 were measured using a blood gas analyzer (ABL800FLEX® Radiometer Corporation, Tokyo, Japan). After the measurements were completed, the oxygen administration method was changed according to the assigned order, and the measurements were repeated in the same manner.
Statistical analysesThe results were analyzed using Friedman repeated measures analysis of variance by ranks with a post hoc Bonferroni test. All statistical analyses were performed with R (The R Foundation for Statistical Computing, Vienna, Austria). Differences were considered significant at a P value of < 0.05. Analysts were blinded to the intervention method.
留言 (0)