
記住我






This is a cross-sectional descriptive-analytical study. According to the Declaration of Helsinki, the Ethical Committee at the Research Center of our University of Medical Sciences approved the study, which has the ethical code IR.IUMS.REC. 1400.640. All questionnaires were filled out in the presence of the examiners.
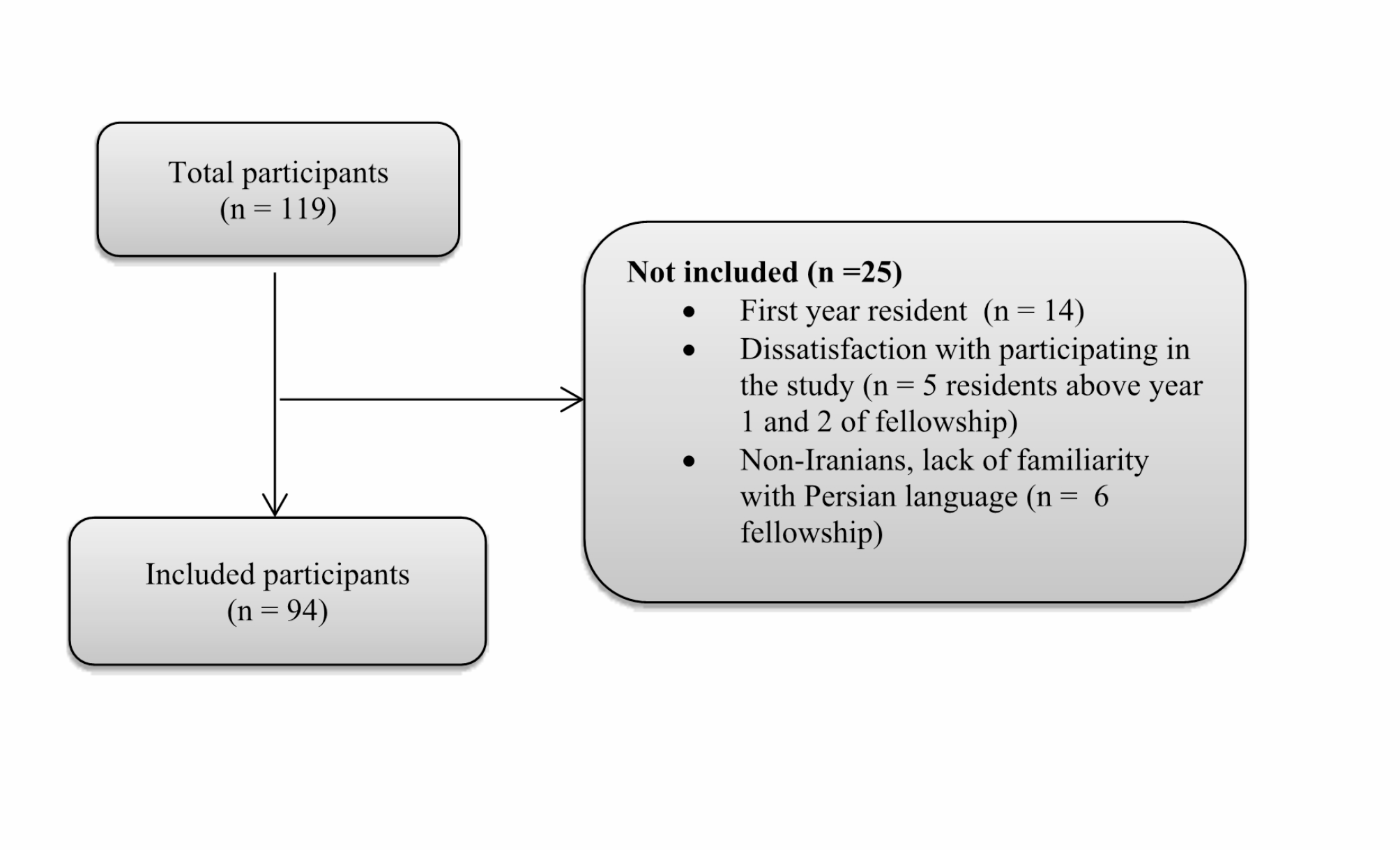
ParticipantsThis study was performed on the 119 orthopedic residents and fellowships in educational-medical hospitals in Tehran, Iran. After excluding 25 people incompatible with the study’s objectives, 94 s-year and above orthopedic residents and fellowships in educational medical hospitals were selected.(Fig. 1).
Fig. 1 Fig. 2
Fig. 2
Distribution of anxiety levels
Inclusion criteria included second-year or higher residents or orthopedic fellowships and informed consent to participate in the study. Non-Iranian orthopedic residents, residents of other specialties, unwillingness to participate in the research, and failure to respond to complete the questionnaires were defined as exclusion criteria.
Demographic questionsThe researcher collected demographic information and participants’ experiences using a checklist. Twelve questions related to demographic characteristics included age, sex, height, weight, family income, marital status, number of children, place of residence, employment status, current income level, having debts to the government, public course status, and correspondence between residence and place of education. Other questions examined participants’ experiences, including job satisfaction, worries about the future, feelings of need for support from responsible organizations, and history of abuse and verbal violence.
Experience questions include two quantitative parts (duration of general medical education, distance between graduates and the start of residency, duration of scientific education related to orthopedics, duration of non-scientific education, duration of hospital stay, weekly duration of work, and average daily sleep hours) and qualitative (Satisfaction with surgeries in the operating room based on the academic year, satisfaction with feedback, feeling the need for social support (insurance), feeling the need for support from nurses in the hospital, concern about the future of employment, desire to continue studying at higher levels, satisfaction From the presence of fellowship in the department, satisfaction with the choice of medical field, satisfaction with the choice of orthopedic assistant field, sufficient authority, balance between work and life, and satisfaction with the income received, the experience of upstream abuse. Qualitative questions were answered on a Likert scale (good, moderate, and poor).
Beck depression inventory II (BDI-II), Beck anxiety inventory (BAI), and stress questionnaireWe used the Beck Depression Inventory-II (BDI-II), Beck Anxiety Inventory (BAI), and the Maslach Burnout Inventory—Human Services Survey (MBI-HSS) to measure subjects’ depression, anxiety, and burnout, respectively. Three questionnaires were filled out according to the standard method described by their authors.
The BDI-II and BAI have 21 questions; the subject must score each question from zero (not at all) to three (very high). This questionnaire’s lowest and highest scores are 0 and 63, respectively. Depression degrees are divided into four groups based on the questionnaire scores: None (0–10), mild (11–16), moderate (20 − 17) and severe (above 21) [20, 21]. Sahebi, Salari, and Asghari (2005) have prepared a Persian version of Beck in Iran and validated it [22]. The internal reliability of the Beck scales was calculated using Cronbach’s alpha, and the following results were obtained: 0.77 for the Depression Scale, 0.79 for the Anxiety Scale, and 0.78 for the Stress Scale. To evaluate the validity of the Beck criterion, the Beck Depression Inventory, Zang Anxiety, and Perceived Stress questionnaires were used simultaneously. The Beck Depression Scale correlation with the Beck Depression Inventory was 0.70, the Beck Anxiety Scale was correlated with the Zang Anxiety Test 0.67, and the Beck Stress Scale correlation with the Perceived Stress Test was 0.49. Factor analysis confirmed the three-factor structure of this questionnaire.
Maslach burnout inventory- Human Services survey (MBI-HSS)The MBI-HSS has 22 questions and estimates burnout at three levels: Emotional Exhaustion (EE), Which contains seven questions; Depersonalization (DP), Which contains seven questions; and low sense of Personal Accomplishment (PA), which Contains eight questions. Each question should be scored between zero (never) to six (every day) in this questionnaire. The range of scores for EE and DP is between 0 and 42, and for CP between 0 and 48. The EE was divided into three levels: low (overall score of 17 or less), moderate (18–29), and high (30 or more). Level classification for DP includes an overall score of 5 or less (low), 6 to 11 (moderate), and an overall score of 12 or higher (High). The CP was divided into three levels: low (Total greater than 40), moderate (34–39), and high (total 33 or less). Cronbach’s alpha coefficient for MBI-HSS was 0.81. A high score in the first two sections and a low score in the last section may indicate burnout [23]. In 2012, Ramin Akbari and colleagues examined the Persian version of the Maslach burnout questionnaire through exploratory and confirmatory factor analysis among 570 English teachers. Their findings showed that this questionnaire can be used in burnout research among Persian-speaking Iranians [23].
Sample size calculationThe appropriate sample size for conducting this study, considering the estimated effect size of 0.23 for the relationship between burnout and depression based on NB Pokhrel, et al. [17] study, with a Type 1 error (α error) of 5% and a power of 80% using G Power version 3.1 statistical software [24], 71 participants were estimated, and to increase the power of the study, all residents and fellowships who met the inclusion criteria at the time of the study were included.
Statistical analysisParticipants’ data were analyzed using SPSS software (version 16(. Subjects were divided into two groups based on questionnaire scores. Subjects with high scores were in Group 1 (participants with high scores for burnout, anxiety, and depression), and those with medium and low scores for questionnaires were in Group 0 )participants with low scores for burnout, anxiety, and depression). The mean ± SD was used to report quantitative variables. Frequency and percentage were used to report qualitative variables. The normality of the distribution of variables was determined via the Kolmogorov–Smirnov test. An Independent t-test was used. If the distribution of variables was not normal, the Mann-Whitney test was applied to compare the variables. Multivariate logistic regression analysis was used to evaluate Burnout-predicting factors. The most important predictors of depression, anxiety, and burnout were estimated using an odds ratio with a 95% confidence interval. P-values less than 0.05 were considered as the significant level of statistical tests.
留言 (0)