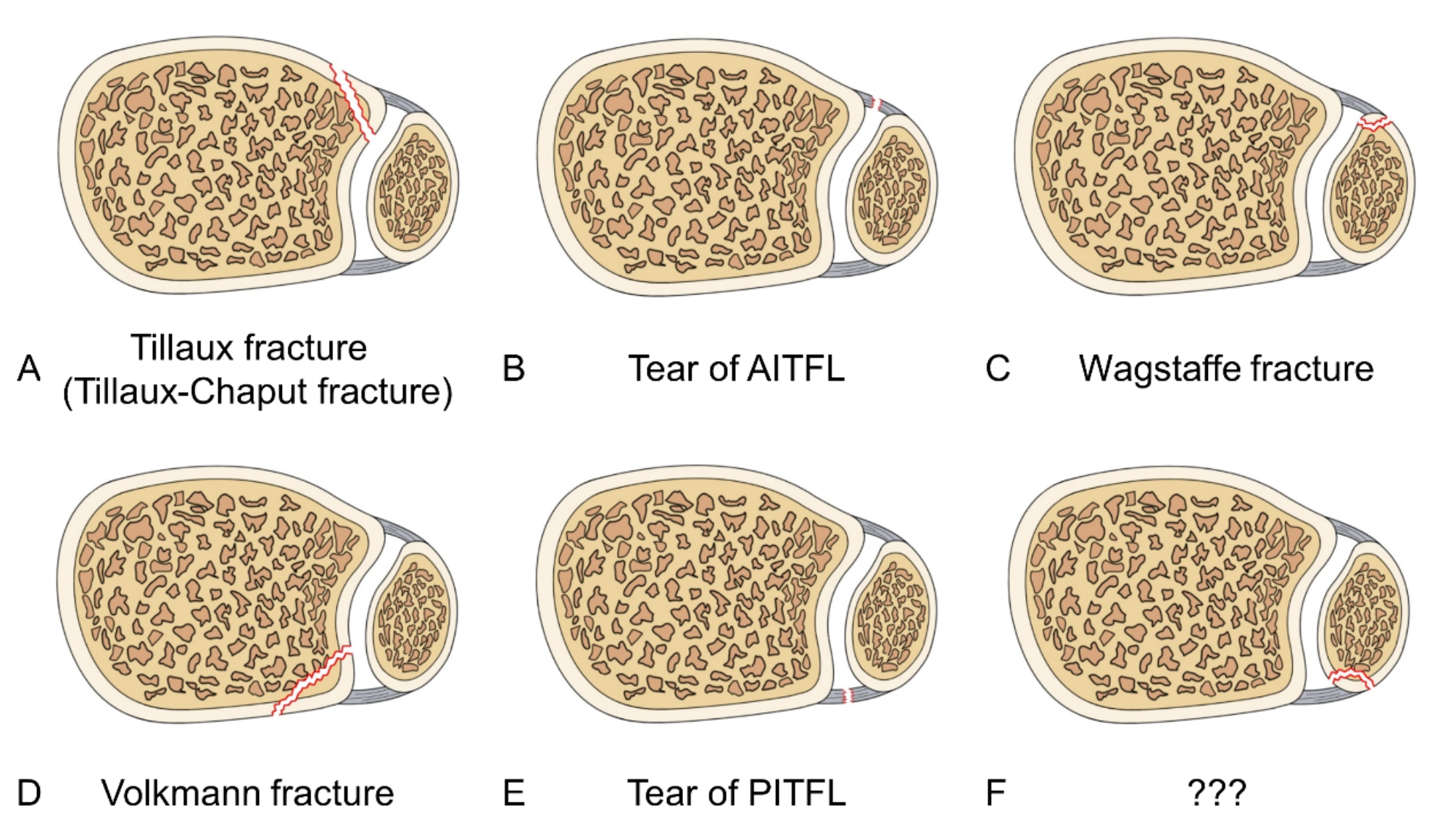
In this study, we analyzed the radiography and CT images of a large sample of patients with ankle fractures and summarized the characteristics of four specific avulsions of the AITFL/PITFL. We detected avulsions of the AITFL/PITFL in 465 out of 1,770 ankle fractures, with a total incidence of 26.3%. Avulsions at the four insertions were most commonly found in supination-external rotation fractures, which accounted for approximately two-thirds (39/93, 39.8%) of Tillaux fractures and fibular avulsions of the PITFL, three-quarters (43/59, 72.9%) of Wagstaffe fractures, and two-thirds (231/353, 65.4%) of Volkmann fractures (Table 2). Avulsion of the AITFL/PITFL may occur at one insertion or at multiple insertions. The incidence of avulsion at one insertion was 23.6% (418/1770) and 2.7% (47/1770) at multiple insertions. In this study, avulsions were found at one, two, or three insertions, but there were no cases of avulsion at all four insertions. Most of the avulsions (418/1,770) occurred at one insertion, and the Volkmann fracture had the highest incidence of all four avulsions (19.9%, 353/1,770). This could be attributable to the synergistic effect of the traction of the PITFL and the posterior superior impact of the talus. The incidence of avulsion at two insertions was 2.6% (46/1770), including 23 cases of Tillaux fracture combined with Volkmann fracture (Figs. 2), 20 cases of Wagstaffe fracture combined with Volkmann fracture (Fig. 3), and three cases of Tillaux fracture combined with fibular avulsion of the PITFL (Figs. 4 and 5). Kose et al. reported two cases of isolated adult Tillaux fracture associated with Volkmann fracture and suggested that such fractures are caused by strong external rotation force of the foot [12]. In line with their speculation, in this study, 16 of the cases of Tillaux fracture combined with Volkmann fracture occurred under external rotation force. Moreover, a similar case of Tillaux fracture occurring in combination with Volkmann fracture as a result of external rotation force was also reported by Mansur et al. [13].
Table 2 Demographic characteristics of patients with avulsionsThe Tillaux fracture appears on CT images as a small fragment of the anterior tibiofibular ligament breaking off from its attachment on the anterolateral tibia. Stefan et al.. proposed that Tillaux-Chaput fractures can be divided into three types: (1) extra-articular avulsion of the AITFL; (2) fracture of the anterolateral tibia involving the joint and tibial incisura; and (3) fracture with impaction of the anterolateral tibial plafond [14]. Tillaux fractures are most common in adolescents between 12 and 14 years of age [15], and it is therefore also referred to as juvenile Tillaux fracture. It represents a transitional subset of Salter-Harris type III fractures of the anterolateral tibial epiphysis [16]. Previous studies have shown that the incidence of Tillaux fractures in adolescents is 5.2–10.0% [17]. However, the incidence of isolated Tillaux fractures in adults has not been reported to date. There have only been a few case reports of adult Tillaux fractures in the literature. Syed et al. [18]., Mishra et al. [19]., and Millan et al. [20]. reported 1 case each of adult Tillaux fracture, and Pereira et al.. reported 2 cases of isolated adult Tillaux fracture [21]. In our study, we identified 93 patients with concomitant Tillaux fractures among the 1,770 ankle fractures, with an incidence of 5.3%. Tillaux fractures were found to occur in conjunction with Volkmann fractures (20 cases) and fibular avulsions of PITFL (3 cases), but there were no cases of combined Wagstaffe fractures. Based on our data, the incidence of Tillaux fractures in adults appears to be significantly lower than that in adolescents. This discrepancy can be attributed to adults having reached full skeletal maturity, as a result of which there is no vulnerable area in the point at which the epiphysis connects with the bone shaft. Thus, when the adult ankle joint is subjected to external forces, the AITFL is more likely to tear than to avulse at its insertion [22]. Tillaux fractures are not easily detected on radiographic images, and it has been suggested that oblique ankle views should be obtained in patients with suspected fracture, along with stress radiography and magnetic resonance imaging to aid in the diagnosis if necessary [23]. Shrestha reported a case of a Tillaux-Chaput fracture diagnosed by ultrasonography and pointed out that the key to diagnosing a fracture by ultrasonography lies in recognizing the cortical discontinuity along the surface of the bone [24]. The treatment of Tillaux fractures is dependent on the size of the bone mass and the degree of displacement. Tillaux fractures with less than 2 mm of displacement can be treated in a conservative way. However, when fragment displacement is > 2 mm or translation is > 1 mm, the patient requires open reduction and internal fixation, including arthroscopic-assisted treatment [25], screw fixation [26], and tension band fixation [27]. A recent study indicates that suture button fixation may yield better outcomes compared to syndesmotic screw fixation [28].
On CT, the Wagstaffe fracture presents as an avulsion fragment of the anteromedial aspect of the distal fibula, which must be distinguished from an avulsion of the lateral collateral ligament. To identify a Wagstaffe fracture, it needs to be considered in conjunction with the patient’s medical history and physical examination, and the use of 3D CT can lead to more accurate identification of such injuries. Wagstaffe classified the Wagstaffe fracture into three types: type I, displaced avulsion fracture of the distal end of the fibula; type II, fracture of the anterior spike of the proximal fibular fragment; type III, fractures of the anterior tubercles from both the tibia and fibula [6]. Wagstaffe fracture often occurs concomitantly with other ankle injuries, such as medial malleolus fractures and fibula fractures [29], with its incidence ranging from 2.7% [29] to 26.5% [30]. Park et al.. reported 13 cases of Wagstaffe fracture, with an incidence of 25% (13/52) [31], and Fisher et al.. reported 40/151 (26.5%) cases [30]. In this study, a total of 59 Wagstaffe fractures were found of which 1 (0.1%, 1/1,770) was classified as type I and 58 (3.3%/1,770) were classified as type II. Wagstaffe fractures were found to occur in conjunction with Volkmann fractures (20 cases), while there were no cases of Tillaux fractures combined with fibular avulsions of the PITFL. The incidence of Wagstaffe fractures in our study was 3.3% (59/1,770), which is lower than that reported in previous studies. This is probably attributable to the large sample size used in this study and the fact that we analyzed all types of ankle fractures rather than only a single type. With regard to the management of Wagstaffe fractures, the size of the fragment influences the fixation method. When the fragment is 5 mm or larger, it needs to be fixed directly, and a non-absorbable suture, Kirschner wire, or single screw can be used for fixation [32].
Volkmann fracture presents as a posterior-lateral avulsion fragment of the distal tibia that is primarily caused by excessive pulling of the PITFL and posterior and superior impact on the talus. The shape and size of a posterior malleolus fracture can often only be determined by spiral CT 3D reconstruction technology. The Volkmann fracture is a type of posterior malleolus fracture that can be classified under Haraguchi type I fractures and accounts for 67% of all posterior malleolus fractures [8]. Volkmann fractures have been rarely reported to occur in isolation in previous studies. Heim et al.. reported 36 cases of Volkmann fracture and discussed its treatment methods [33]. In this study, Volkmann fractures were observed in 353 out of 1,770 adult ankles, with an incidence of 19.9%, which was the highest among the four insertions around the tibiofibular syndesmosis. Volkmann fractures occurred in conjunction with Tillaux fractures (23 cases) and Wagstaffe fractures (20 cases), but no cases of Volkmann fractures combined fibular avulsions of the PITFL were found. The treatment of Volkmann fractures is dependent on the size of the fragment and the degree of displacement. When the posterior fragment is < 10% of the distal articular surface, the treatment is mainly conservative. However, when the posterior fragment is > 25% of the articular surface or displaced by > 2 mm, it is treated with open reduction and internal fixation [34]. It has been suggested that a fragment in the size range of 10–25% does not require fixation of the posterior ankle if the articular surface is flat. However, posterior fragment fixation was reported to contribute to functional outcomes by decreasing the incidence of articular step-off of > 1 mm [35]. Therefore, it might be beneficial in the management of Volkmann fractures. Fixation of Volkmann fracture can be achieved with screws [36] and plates [8]. Ahmed et al. advocated that in cases of posterior malleolus fractures accompanied by syndesmotic diastasis, the posterior malleolus should be fixed first, as this approach may eliminate the need for syndesmotic screws [37]. Giordano et al.. suggested that for fragments with 10% involvement of the tibiotalar articular surface, the use of a trans-syndesmotic screw is sufficient, but when the involvement is greater than 25%, either a non-locked or a locked plate must be used to buttress the tibial posterior malleolus. In posterior fragments with 45% involvement, the use of a locking plate is recommended [34].
A remarkable finding in this study is that there were 8 (0.5%) cases of fibular avulsion of the PITFL among the 1,770 adult ankle fractures. To our knowledge, this is the first report of this type of fracture in the current literature. This avulsion appeared as a posterior medial avulsion fragment of the distal fibula on CT images, but lacked specificity on radiographic images. In our study, all eight cases of fibular avulsion fractures of PITFL were diagnosed by CT imaging (including two-dimensional and three-dimensional). Among the 8 patients, there were 5 males and 3 females, with an average age of 58.5 ± 11.0 years. According to the Weber-AO classification system, there were three cases of type A, three cases of type B, and two cases of type C fractures. According to the Lauge-Hansen classification system, there were three cases of supination-adduction type fractures, three cases of supination external rotation type fractures, and two cases of pronation external rotation type fractures (Table 3). Three of the eight cases were associated with Tillaux-Chaput fractures and five were isolated. Six of the eight patients were treated surgically, and two were treated conservatively with cast immobilization. Six of the eight patients underwent surgery, but none underwent targeted fixation of the bone fragment. Further, three of the eight fibular avulsions of the PITFL were accompanied with Tillaux fractures (Figs. 4 and 5).
Table 3 Demographic characteristics of patients with fibular avulsion of the PITFLFibular avulsion of the PITFL is theoretically similar to the Volkmann fracture, which is also caused by separation of the tibiofibular syndesmosis. According to Neer’s ring theory [38], a fibular avulsion of the PITFL also implies disruption of the integrity of the ankle joint ring. When missed or left untreated, this avulsion fracture may lead to ankle instability, pain, and other complications, which may affect the restoration of normal ankle joint anatomy and function. Appropriate management of this newly identified fracture type will certainly contribute to the stability of the lower tibiofibular syndesmosis of the ankle. Neither the Weber-AO or Lauge-Hansen classification describe the morphology or injury mechanism of this type of fracture. Thus, a more comprehensive classification system of ankle fractures that includes this avulsion fracture is required. Regrettably, due to its extremely low incidence, the treatment strategy for this type of fracture is unclear and warrants further research.







留言 (0)