
記住我






Institutional review board approval was obtained from the ethics committee of our hospital, and informed consent was acquired from all included patients before the commencement of this retrospective study. The medical records of the patients with unilateral recurrent patellar subluxation who underwent DDFO between January 2014 and June 2019 at our hospital were identified and reviewed. The inclusion criteria were: (1) at least one episode of patellar subluxation; (2) at least one symptom of patellar instability (pain, subluxation, or both) for more than 3 months; (3) femoral torsion > 30°; (4) skeletal maturity.
The exclusion criteria were: (1) Tibial tuberosity-trochlear groove (TT-TG) distance > 20 mm; (2) high grade trochlear dysplasia (grades B, C or D) according to Dejour’s classification [4]; (3) patella alta with Caton-Deschamps index > 1.2; (4) malalignment of the lower limb (> 5° varus or valgus); (5) generalized or localized joint laxity; (6) fracture around the knee; (7) habitual or traumatic dislocation; (8) previous knee surgery; (9) concomitant ligament reconstruction (collateral ligaments or cruciate ligaments); (10) revision surgery. Patients with criteria (1) to (3) had to receive other bony procedures, and thus were excluded. Patients with patellofemoral osteoarthritis, osteonecrosis, rheumatoid arthritis, and other disorders that seriously impaired neuromuscular function were also excluded. Based on above-mentioned criteria, 76 patients were included from a total of 145 reviewed patients. All patients were followed up for at least 3 years.
To identify the characteristics of femoral torsion and establish the new classification system for patients with recurrent patellar subluxation and excessive femoral torsion, 40 patients with isolated meniscus or soft tissue injury were recruited as the control group. Demographic and clinical data were collected from the medical records, including gender, age, height, and weight.
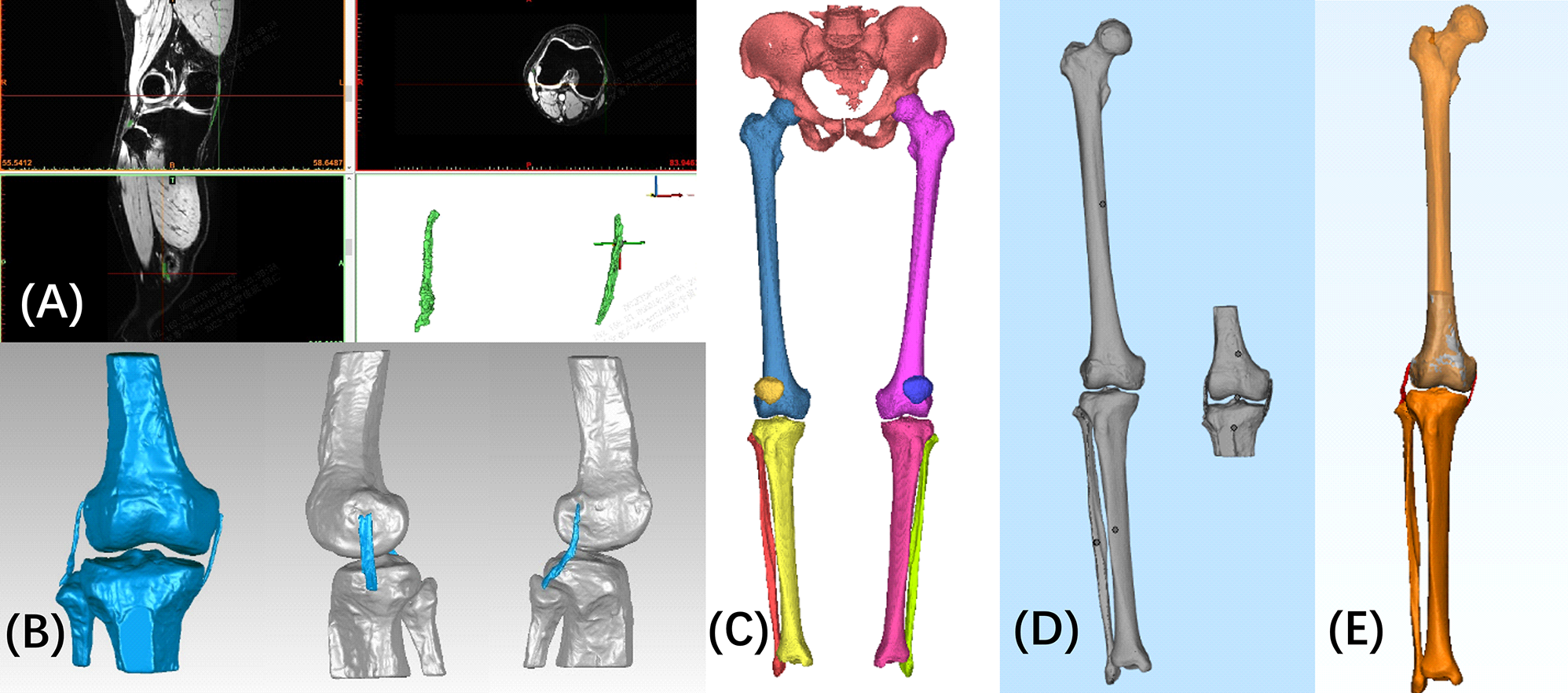
Parameters of femoral torsionThe measurement of segmental torsion of the femur (neck, shaft, and distal femur) was described and verified by Ferlic et al [5] and Chen et al [3] using four lines in four different segments on computed tomography (CT) images (Fig. 1). The first line (proximal femur axis, PFA) was drawn through the center of the femoral head and neck on the slices showing the entire femoral head and neck. The second line (lesser trochanter line, LTL) was drawn through the center of the femoral shaft and the midpoint of the lesser trochanter at its greatest prominence. The third line (distal femur shaft line, DFSL) was defined by a tangent to the posterior aspect of the distal femur on the slice just proximal to the attachment of the gastrocnemius heads. The fourth line (posterior condylar line, PCL) was drawn tangent to the medial and lateral posterior condyles on the slice showing the intact “Roman Arch”. The parameters of femoral torsion were evaluated by the angles formed between these lines. Neck torsion was formed between PFA and LTL. Shaft torsion was formed between LTL and DFSL. Distal torsion was formed between DFSL and PCL. The total femoral torsion was measured between PFA and PCL.
Fig. 1
The measurement of the segmental torsion of the femur. A Proximal femur axis. B Lesser trochanter line. C Distal femur shaft line. D Posterior condylar line
Classification criteriaThis study developed a novel classification system for patients with recurrent patellar subluxation and excessive femoral torsion according to the femoral torsion segment which contributed most to the total femoral torsion. The new classification system included two types. Type I was defined as the proximal torsion in which neck and shaft segments contributed most to total femoral torsion. Type II was defined as the distal torsion in which distal femur segment contributed most to total femoral torsion.
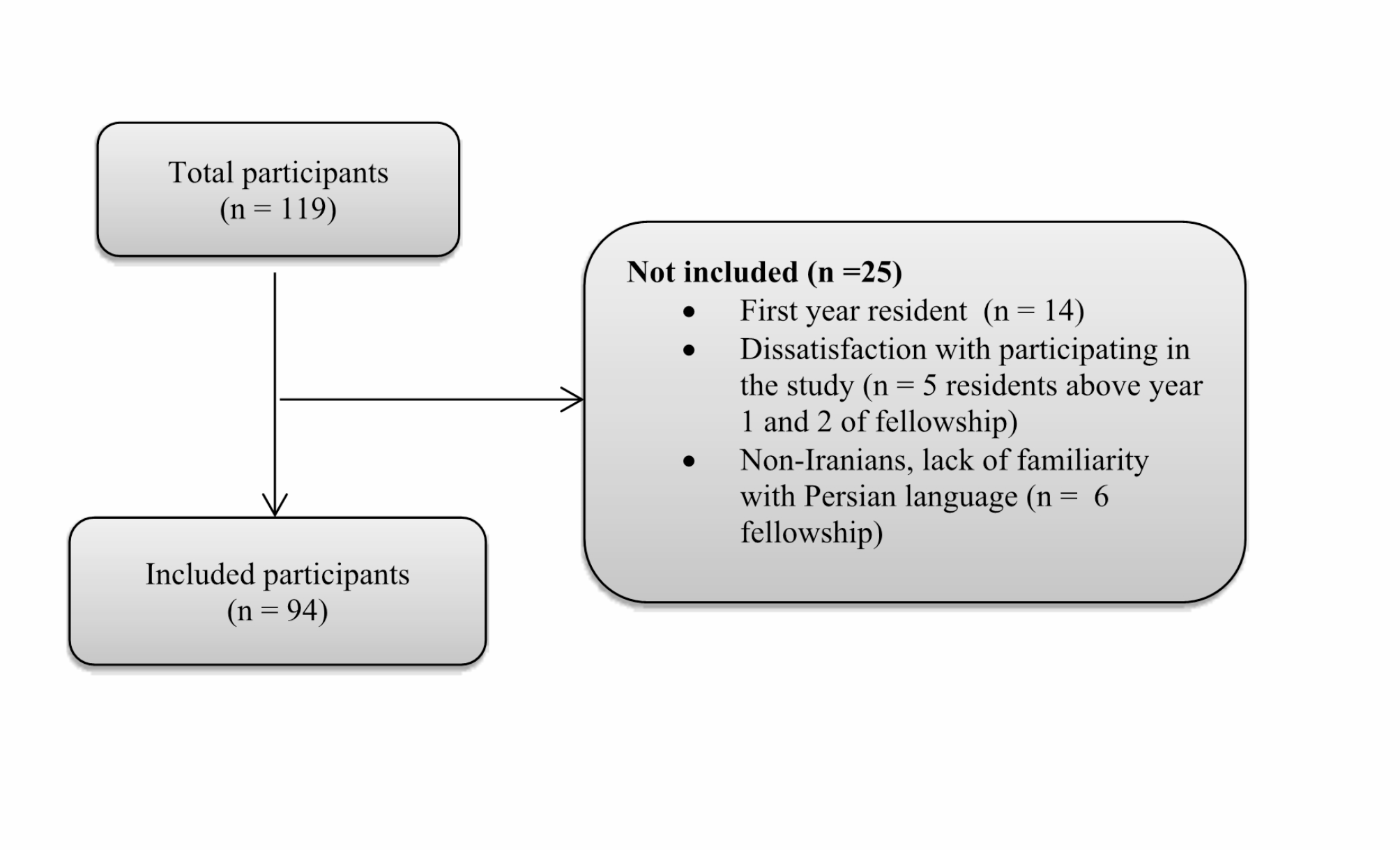
Patients included with recurrent patellar subluxation and excessive femoral torsion were further classified into two groups according to this classification. The proximal torsion group comprised 36 patients with type I femoral torsion, and the distal torsion group comprised 40 patients with type II femoral torsion. Three patients were lost to follow-up, leading to 35 patients in the proximal torsion group and 38 patients in the distal torsion group (Fig. 2). Patient demographics and clinical data were shown in Table 1. There was no significant difference among the three groups regarding these parameters.
Fig. 2
Flowchart of the patient selection in proximal torsion group and distal torsion group. DDFO, derotational distal femoral osteotomy; TT-TG, tibial tuberosity-trochlear groove
Table 1 Patient demographics and clinical data in proximal torsion group, distal torsion group, and control groupαSurgical techniqueAll patients included in the torsion groups received DDFO combined with medial patellofemoral ligament reconstruction (MPFLR) performed by the same experienced senior surgeon. The DDFO was performed on the lateral thigh along the longitude axis of the distal femur. The distal femoral shaft was exposed through the intermuscular space. The supracondylar osteotomy line was set parallel to the tibiofemoral joint line. Then the Kirschner wires were inserted into osteotomy line to determine the rotational angle, which was based on the preoperative measurement, and was verified by intraoperative fluoroscopy. The distal femur was externally rotated to the predetermined angle, and fixed using a lateral Tomofix distal femoral plate with locking screws (DePuy Synthes, Umkirch, Germany) after checking the reduction of the femur through fluoroscopy.
The double-bundle anatomic MPFLR was performed using ipsilateral gracilis tendon prepared in a Y shape. The femoral and patellar tunnels were located according to the native MPFL anatomy [24]. The position of the femoral tunnel was based on the osseous landmarks between the adductor tubercle and the medial femoral epicondyle, which was verified using fluoroscopy [11]. Two patellar tunnels were drilled in the upper corner and the center of the medial edge of the patella. The gracilis tendon was passed through the tunnels, and fixed in the femoral tunnel at 90° of knee flexion. Further release of the lateral retinaculum was performed if there was tightness. The preoperative and postoperative radiographs and CT images in the proximal torsion group and distal torsion group were shown in Figs. 3 and 4.
Fig. 3
The preoperative and postoperative radiographs in the A proximal torsion group and B distal torsion group
Fig. 4
The preoperative and postoperative computed tomography images in the A proximal torsion group and B distal torsion group
Postoperative rehabilitationAll patients received a standard phase-based rehabilitation protocol, including weightbearing exercise, range of motion (ROM) training, and quadriceps muscle strength exercise. Patients were required to wear knee braces in full extension during the first 6 weeks after surgery. Full weightbearing exercise was permitted at 6 weeks after surgery. The ROM was gradually increased to 90° in the first 2 weeks, and to 120° in the following 4 weeks. The quadriceps muscle strength exercise was encouraged early after surgery. Daily activities were allowed after 2 months, and sports such as jogging and running were allowed after 3 months if the muscle strength had been fully recovered.
Clinical evaluationClinical evaluation was performed before and 3 years after surgery, including functional outcome, physical examination, quality of life, activity level, satisfaction, and complication. Physical examination consisted of patellar apprehension test and ROM. Functional outcomes included Kujala score, Lysholm score, and International Knee Documentation Committee (IKDC) subjective knee evaluation score [8, 15, 19]. Quality of life was evaluated using the five-level EuroQol five-dimensional questionnaire (EQ-5D-5L), and the vertical visual analogue scale (EQ-VAS) [9, 20]. The activity level was evaluated using the Tegner activity score and rate of return to sports [26]. Patients were asked whether they returned to the same, lower, or higher level of activities compared with preoperative level, and the reasons not returning to sports. Satisfaction was evaluated and further divided into four levels: very satisfied, satisfied, partially satisfied, and not satisfied at all. The recurrence of subluxation/dislocation, and other complications, such as nonunion of the osteotomy area, anterior knee pain, stiffness, and patellar fracture, were recorded during the follow-up.
Radiological evaluationRadiological evaluation was performed within 1 week before surgery and at 3 years after surgery, including patellofemoral osteoarthritis, alignment, and congruence. Patellofemoral osteoarthritis was assessed routinely using patellar skyline views taken at knee flexion of 45°, which was graded according to the Iwano classification with grades I-IV [11]. Patellofemoral alignment was evaluated using the TT-TG distance measured between two lines perpendicular to the PCL on two overlapped axial CT slices. One line was drawn from the deepest point of the trochlear sulcus, and another line was drawn from the center of the tibial tuberosity on the slice showing approximately proximal one-third of the tibial tuberosity. [21]
Patellofemoral congruence was evaluated using patella tilt angle (PTA), patellar congruence angle (PCA), and patella-trochlear groove distance (PTGD) on axial CT images (Fig. 5). The PTA was measured between the maximum width axis of the patella and the PCL [14]. The PCA was measured between the line passing through the lowest point of the patella and the deepest point of the sulcus, and the line bisecting sulcus angle that formed by the tangent lines of medial and lateral articular aspects of the trochlea [28]. The PTGD was defined as the distance between the perpendicular line of the PCL passing through the deepest point of the sulcus, and the medial margin of the patella [30]. The tibial torsion angle was formed between the line passing through the midpoints of the medial and lateral malleoli, and the line tangent to the posterior margin of the tibial plateau. [22]
Fig. 5
The measurement of patellofemoral congruence. A Patella tilt angle. B Patellar congruence angle. C Patella-trochlear groove distance
Measurements of parametersAll measurements were performed by 2 independent researchers who were blinded to the patient grouping and research hypothesis in a randomized fashion to determine inter-observer reliability. The average values were used in the final analysis. To evaluate intra-observer reliability, one researcher reexamined all the measurements after 6 weeks. The intraclass correlation coefficient (ICC) values were calculated, and the ICC value > 0.8 indicated excellent reliability. All the measured parameters showed excellent inter-observer reliability with ICC values ranging from 0.854 to 0.912, and intra-observer reliability with ICC values ranging from 0.885 to 0.947.
Statistical analysisThe data were described as means and standard deviations for continuous variables, and number and percentage for categorical variables. After normal distribution of all parameters were confirmed using the Kolmogorov–Smirnov test, the differences were analyzed using the two-tailed Student’s t-test between 2 groups or within a group, and one-way analysis of variance (one-way ANOVA) among 3 groups. The chi-square test was performed for the categorical variables. Statistical significance was set at P < 0.05. All statistical analyses were performed with SSPS version 21.0 (SPSS Inc., Chicago, IL, USA) software. G*Power 3 (Heinrich Heine, Universität Düsseldorf, Düsseldorf, Germany) was applied to determine the suitable sample size. An a-priori power analysis with the α < 0.05 and the effect size of 0.8 showed that a minimum number of 34 patients in each group were adequate to detect significant differences with a power of 90%.
留言 (0)