
記住我


Patients in the control group will receive 100 mg of acetylsalicylic acid along with a placebo, both administered in two daily doses. Acetylsalicylic acid is a proven medication for preventing preeclampsia [8].
Intervention description Intervention groupThe intervention groups will be designated as EG I and EG II. Patients in EG I will receive daily doses of 1000 mg of calcium carbonate (commercial grade), divided into two doses of 500 mg, along with 100 mg of acetylsalicylic acid, encapsulated in hard gelatin capsules. Patients in EG II will receive 1000 mg of calcium carbonate derived from Crassostrea sp. oysters, also divided into two doses of 500 mg, alongside 100 mg of acetylsalicylic acid in gelatin capsules.
The calcium carbonate extracted from Crassostrea sp. oyster shells will be developed by the Federal University of Sergipe in collaboration with the Federal University of Alagoas. The handling of capsules will follow the guidelines in the Brazilian Pharmacopoeia (6th ed., 2019) and the Brazilian Technical Response Service (SBRT, 2012). To ensure quality, the capsules will undergo rigorous testing, including evaluations of visual characteristics such as color, deformities, and the presence of foreign particles in the formulation.
In Brazil, calcium carbonate is primarily available as mass-produced capsules from pharmaceutical companies. Although not prohibitively expensive, calcium carbonate capsules are not among the least costly medications. Additionally, the country possesses untapped natural resources, particularly related to sustainable sources [9]. Calcium carbonate can be sourced from mollusk shells found along the Brazilian coast, which are typically discarded and not utilized by fishing communities. These renewable sources are environmentally integrated and, through collaborations between local communities, companies, and universities, calcium carbonate powder from these sources is being evaluated for its purity and pharmacopoeial properties and tested in pharmaceutical formulations [10].
Criteria for discontinuing or modifying allocated interventionsIf patients experience any adverse reactions to the medications, they will be monitored, and, depending on the severity, may be excluded from the study. Additionally, participants retain the right to withdraw from the research at any time, regardless of the reason.
Strategies to improve adherence to interventionsTo improve medication adherence, pharmacists will provide ongoing support, explaining the importance of the treatment and addressing any questions. Weekly phone calls will also be made to each patient to follow up on their treatment progress.
Medication adherence will be measured using the Brief Medication Questionnaire (BMQ), a tool that assesses barriers to adherence, beliefs about the regimen, and recall of drug treatment from the patient’s perspective.
Relevant concomitant care permitted or prohibited during the trialParticipants who were on other medications prior to or during pregnancy will continue their treatments as prescribed, provided these do not interfere with the study interventions. In the event of potential drug-drug interactions, a case-by-case evaluation will be conducted to assess the safety and feasibility of continued participation. Patients will be monitored during each prenatal consultation, where adherence to the study protocol will be assessed. Non-adherence to the allocated intervention will result in withdrawal from the trial.
Provision for post-trial careAll participants who complete the study, whether regularly or prematurely (due to serious adverse effects or ongoing adverse events such as abnormal laboratory results or vital signs), will be referred to the healthcare team for continued monitoring, and full support will be provided.
Outcomes Primary outcomesIncidence of preeclampsia.
Secondary outcomesTable 1 presents maternal and fetal results that may be related to the effects of calcium carbonate and will be observed throughout the study.
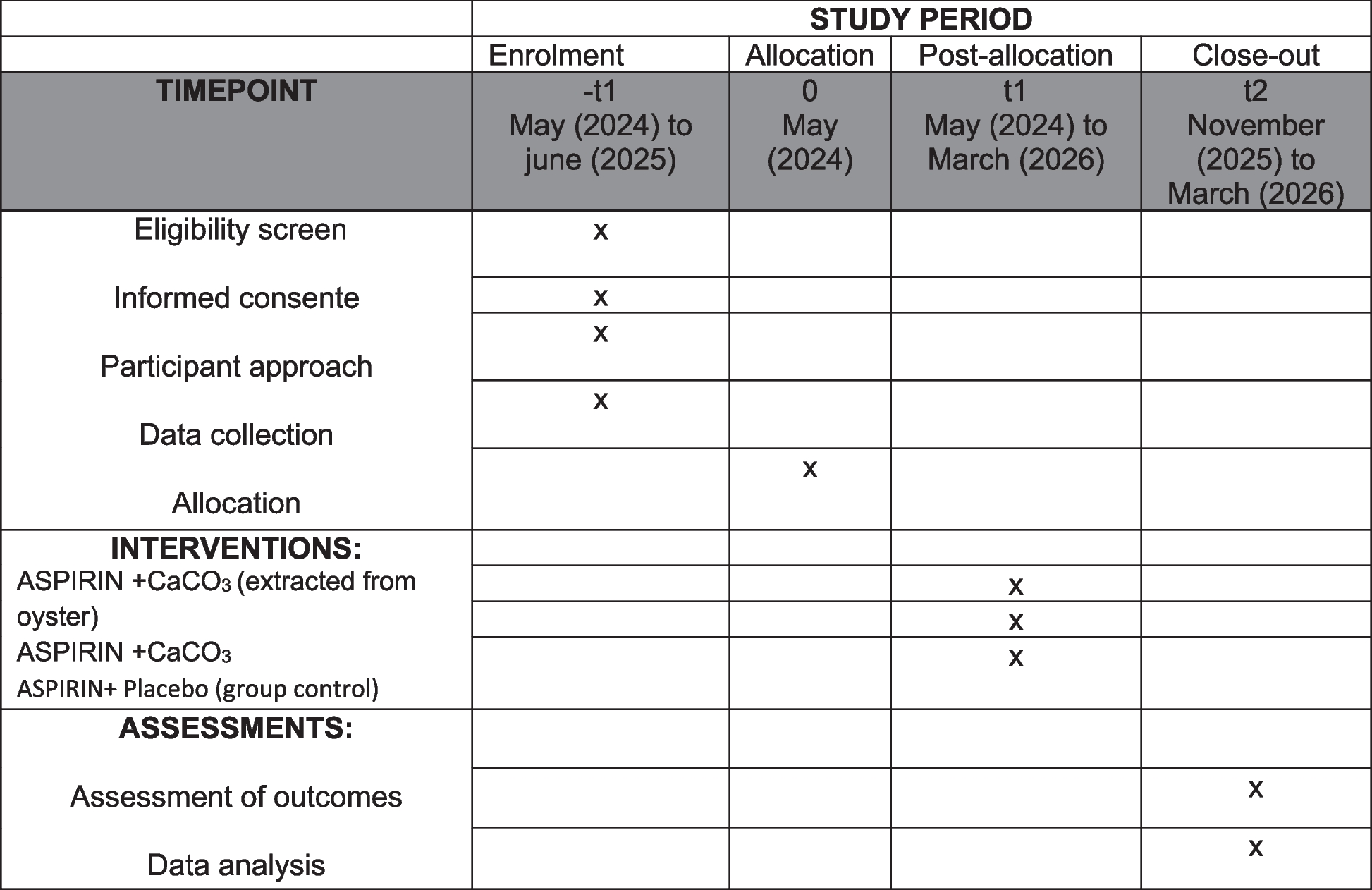
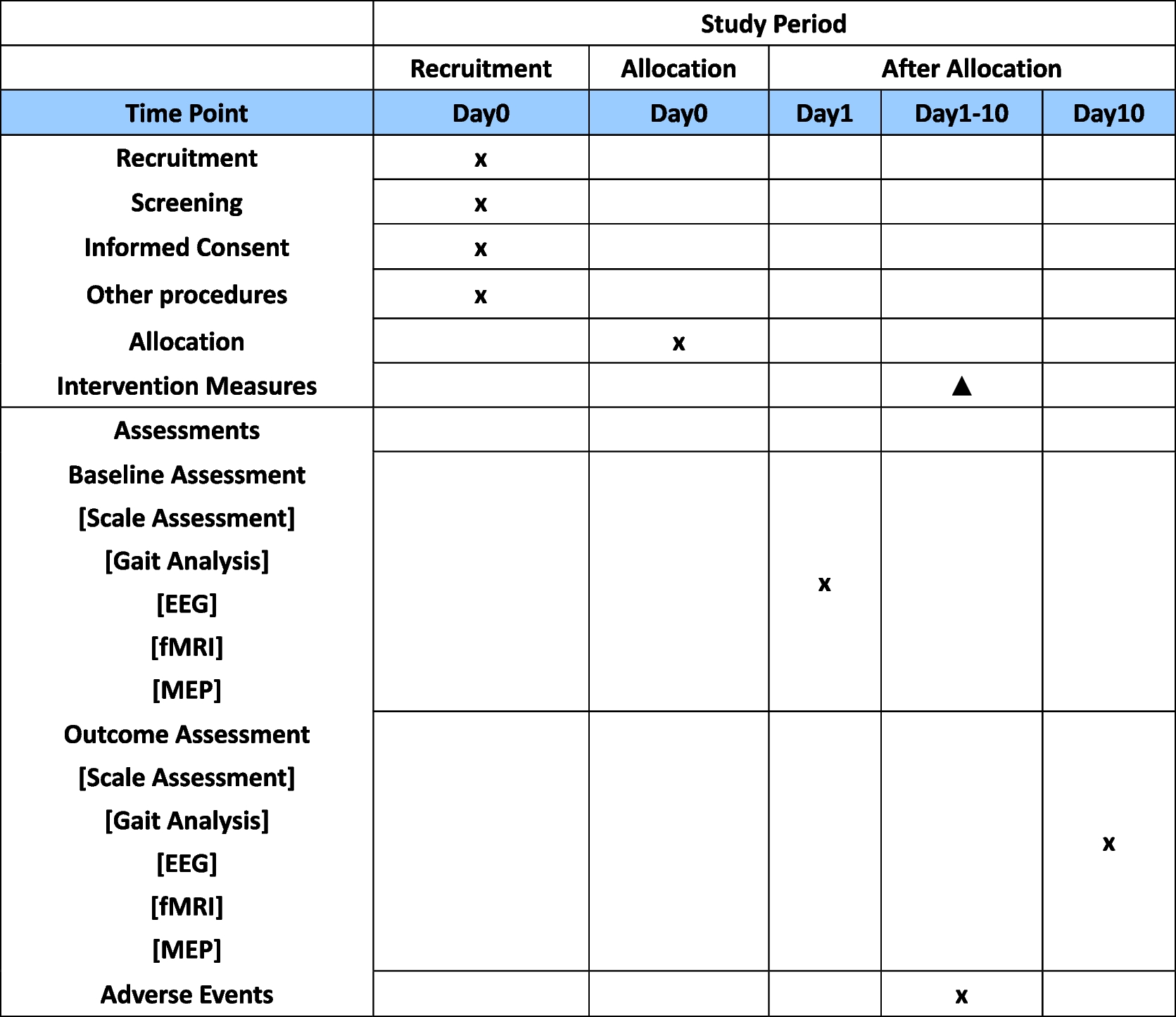
Table 1 Secondary outcomes that may be related to preeclampsiaParticipant timelineData collection will occur from May 2024 to March 2026, with participant recruitment continuing until June 2025. Monitoring will be conducted throughout the entire data collection period. The research steps are outlined in Fig. 1.
Fig. 1
Representation of the data collection stages (SPIRIT figure)
Sample sizeA sample size of at least 156 patients per group was calculated to provide 80% power to detect a 50% reduction in the incidence of preeclampsia (PE), assuming that 30% of high-risk pregnant women will develop PE. A two-sided t-test with a familywise α level of 0.05 will be used. To adjust for multiple comparisons among the three groups, the Sidak correction will be applied, yielding an adjusted α level of approximately 0.017 for each comparison. Considering these adjustments, the total required sample size is approximately 468 participants, with 156 in each of the three groups (two intervention groups and one placebo group). To accommodate an anticipated dropout rate of 10%, the sample size per group is increased to approximately 173 patients. This adjustment ensures that the study will maintain adequate power to detect a statistically significant difference while minimizing the risks of type I and type II errors.
RecruitmentParticipants will be systematically approached at the prenatal care facility and invited to participate in the study. The research procedures will be thoroughly explained to all potential participants before enrollment.
留言 (0)